



Malcolm Tan
@ibdgastrodocsg.bsky.social
Gastroenterologist | IBD Service Director | Singapore General Hospital.
Pinned
Obefazimod in mod-severe UC
- week 8 induction data presented at #UEGWeek
- first in class for IBD
1/🧵
MoA: ⬆️expression of miR-124, which regulates inflammatory response & restores mucosal homeostasis.
- week 8 induction data presented at #UEGWeek
- first in class for IBD
1/🧵
MoA: ⬆️expression of miR-124, which regulates inflammatory response & restores mucosal homeostasis.

October 20, 2025 at 1:48 AM
Obefazimod in mod-severe UC
- week 8 induction data presented at #UEGWeek
- first in class for IBD
1/🧵
MoA: ⬆️expression of miR-124, which regulates inflammatory response & restores mucosal homeostasis.
- week 8 induction data presented at #UEGWeek
- first in class for IBD
1/🧵
MoA: ⬆️expression of miR-124, which regulates inflammatory response & restores mucosal homeostasis.
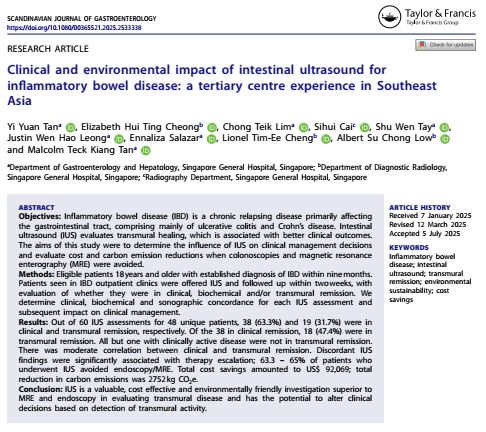
How intestinal ultrasound (IUS) changes IBD care – clinical impact, cost savings & greener healthcare
1/ #IBD is rising fast in SE Asia 📈
We need tools that are accurate, patient-friendly, and sustainable.
Our SGH pilot study shows #IntestinalUltrasound ticks all 3 boxes ✅
1/ #IBD is rising fast in SE Asia 📈
We need tools that are accurate, patient-friendly, and sustainable.
Our SGH pilot study shows #IntestinalUltrasound ticks all 3 boxes ✅
August 10, 2025 at 6:31 AM
How intestinal ultrasound (IUS) changes IBD care – clinical impact, cost savings & greener healthcare
1/ #IBD is rising fast in SE Asia 📈
We need tools that are accurate, patient-friendly, and sustainable.
Our SGH pilot study shows #IntestinalUltrasound ticks all 3 boxes ✅
1/ #IBD is rising fast in SE Asia 📈
We need tools that are accurate, patient-friendly, and sustainable.
Our SGH pilot study shows #IntestinalUltrasound ticks all 3 boxes ✅
APOLLO-CD
A phase 2a induction trial of tulisokibart, an anti-TL1A monoclonal antibody, shows promising efficacy & safety in patients with moderate-to-severe Crohn’s disease (CD) refractory to prior therapies.
Key findings from the APOLLO-CD study:
[🔗https://doi.org/10.1016/S2468-1253(25)00071-8]
A phase 2a induction trial of tulisokibart, an anti-TL1A monoclonal antibody, shows promising efficacy & safety in patients with moderate-to-severe Crohn’s disease (CD) refractory to prior therapies.
Key findings from the APOLLO-CD study:
[🔗https://doi.org/10.1016/S2468-1253(25)00071-8]
June 27, 2025 at 7:56 AM
APOLLO-CD
A phase 2a induction trial of tulisokibart, an anti-TL1A monoclonal antibody, shows promising efficacy & safety in patients with moderate-to-severe Crohn’s disease (CD) refractory to prior therapies.
Key findings from the APOLLO-CD study:
[🔗https://doi.org/10.1016/S2468-1253(25)00071-8]
A phase 2a induction trial of tulisokibart, an anti-TL1A monoclonal antibody, shows promising efficacy & safety in patients with moderate-to-severe Crohn’s disease (CD) refractory to prior therapies.
Key findings from the APOLLO-CD study:
[🔗https://doi.org/10.1016/S2468-1253(25)00071-8]
2025 guidelines for IBD from @amcollegegastro.bsky.social
Crohn's: journals.lww.com/ajg/fulltext...
UC: journals.lww.com/ajg/fulltext...
#IBDSky #MedSky #GISky
Crohn's: journals.lww.com/ajg/fulltext...
UC: journals.lww.com/ajg/fulltext...
#IBDSky #MedSky #GISky




June 21, 2025 at 12:21 AM
2025 guidelines for IBD from @amcollegegastro.bsky.social
Crohn's: journals.lww.com/ajg/fulltext...
UC: journals.lww.com/ajg/fulltext...
#IBDSky #MedSky #GISky
Crohn's: journals.lww.com/ajg/fulltext...
UC: journals.lww.com/ajg/fulltext...
#IBDSky #MedSky #GISky
Checkpoint inhibitor-induced colitis (ICI-colitis): a serious, often under-recognized complication in cancer patients receiving immunotherapy.
1/ ICI-induced colitis
📈 Affects up to 30% of patients on ICIs.
🔬 This study followed 96 patients with 12-month outcomes.
www.esmoopen.com/article/S205...
1/ ICI-induced colitis
📈 Affects up to 30% of patients on ICIs.
🔬 This study followed 96 patients with 12-month outcomes.
www.esmoopen.com/article/S205...
June 2, 2025 at 3:10 AM
Checkpoint inhibitor-induced colitis (ICI-colitis): a serious, often under-recognized complication in cancer patients receiving immunotherapy.
1/ ICI-induced colitis
📈 Affects up to 30% of patients on ICIs.
🔬 This study followed 96 patients with 12-month outcomes.
www.esmoopen.com/article/S205...
1/ ICI-induced colitis
📈 Affects up to 30% of patients on ICIs.
🔬 This study followed 96 patients with 12-month outcomes.
www.esmoopen.com/article/S205...




May 4, 2025 at 2:21 AM
BSG 2025 Guidelines: Colorectal Surveillance in IBD
gut.bmj.com/content/earl...
@bmj.com #GISky #IBDSky
gut.bmj.com/content/earl...
@bmj.com #GISky #IBDSky




May 1, 2025 at 8:02 AM
BSG 2025 Guidelines: Colorectal Surveillance in IBD
gut.bmj.com/content/earl...
@bmj.com #GISky #IBDSky
gut.bmj.com/content/earl...
@bmj.com #GISky #IBDSky


ADMIT-ASC index for ASUC.
Score of ≥3 was 84% predictive of steroid failure
- CRP ≥100mg/L (1 point)
- albumin ≤25g/L (1 point)
- UCEIS ≥4 (1 point) or ≥7 (2 points)
Will these pts benefit from early 'salvage' therapy instead of waiting till Day 3?
#IBDSky #GISky
gut.bmj.com/content/72/3...
Score of ≥3 was 84% predictive of steroid failure
- CRP ≥100mg/L (1 point)
- albumin ≤25g/L (1 point)
- UCEIS ≥4 (1 point) or ≥7 (2 points)
Will these pts benefit from early 'salvage' therapy instead of waiting till Day 3?
#IBDSky #GISky
gut.bmj.com/content/72/3...


April 14, 2025 at 6:02 AM
ADMIT-ASC index for ASUC.
Score of ≥3 was 84% predictive of steroid failure
- CRP ≥100mg/L (1 point)
- albumin ≤25g/L (1 point)
- UCEIS ≥4 (1 point) or ≥7 (2 points)
Will these pts benefit from early 'salvage' therapy instead of waiting till Day 3?
#IBDSky #GISky
gut.bmj.com/content/72/3...
Score of ≥3 was 84% predictive of steroid failure
- CRP ≥100mg/L (1 point)
- albumin ≤25g/L (1 point)
- UCEIS ≥4 (1 point) or ≥7 (2 points)
Will these pts benefit from early 'salvage' therapy instead of waiting till Day 3?
#IBDSky #GISky
gut.bmj.com/content/72/3...
SES-CD for Crohn's
4 parameters:
- size of ulcers
- extent of ulcerated surface
- extent of colitis
- stenosis
5 segments:
- ileum, right, transverse, left colon and rectum
Endo remission: ≤2 (or <4)
Accessible online calculator: www.e-guide.ecco-ibd.eu/resources/ca...
#IBDSky #GISky #SurgSky
4 parameters:
- size of ulcers
- extent of ulcerated surface
- extent of colitis
- stenosis
5 segments:
- ileum, right, transverse, left colon and rectum
Endo remission: ≤2 (or <4)
Accessible online calculator: www.e-guide.ecco-ibd.eu/resources/ca...
#IBDSky #GISky #SurgSky

April 14, 2025 at 6:01 AM
SES-CD for Crohn's
4 parameters:
- size of ulcers
- extent of ulcerated surface
- extent of colitis
- stenosis
5 segments:
- ileum, right, transverse, left colon and rectum
Endo remission: ≤2 (or <4)
Accessible online calculator: www.e-guide.ecco-ibd.eu/resources/ca...
#IBDSky #GISky #SurgSky
4 parameters:
- size of ulcers
- extent of ulcerated surface
- extent of colitis
- stenosis
5 segments:
- ileum, right, transverse, left colon and rectum
Endo remission: ≤2 (or <4)
Accessible online calculator: www.e-guide.ecco-ibd.eu/resources/ca...
#IBDSky #GISky #SurgSky


GRAVITI trial 🧵
Guselkumab is an IL-23 inhibitor.
GRAVITI tested fully SC dosing (no IV) for both induction & maintenance in moderate-to-severe Crohn’s.
N = 347 adults, randomized 1:1:1
- GUS 400 mg q4w induction → 100 mg q8w
- GUS 400 mg q4w induction → 200 mg q4w
#IBDSky #GISky #MedSky
Guselkumab is an IL-23 inhibitor.
GRAVITI tested fully SC dosing (no IV) for both induction & maintenance in moderate-to-severe Crohn’s.
N = 347 adults, randomized 1:1:1
- GUS 400 mg q4w induction → 100 mg q8w
- GUS 400 mg q4w induction → 200 mg q4w
#IBDSky #GISky #MedSky



April 14, 2025 at 5:56 AM
Can removing the appendix help prevent relapse in ulcerative colitis?
The #ACCURE trial says: Yes. 🧵
✂️ Pragmatic, open-label RCT across 22 centers (Netherlands, UK, Ireland).
Patients in UC remission randomized to:
✅ Appendicectomy + standard medical therapy
vs
🧪 Standard medical therapy alone
The #ACCURE trial says: Yes. 🧵
✂️ Pragmatic, open-label RCT across 22 centers (Netherlands, UK, Ireland).
Patients in UC remission randomized to:
✅ Appendicectomy + standard medical therapy
vs
🧪 Standard medical therapy alone


April 14, 2025 at 5:20 AM
Can removing the appendix help prevent relapse in ulcerative colitis?
The #ACCURE trial says: Yes. 🧵
✂️ Pragmatic, open-label RCT across 22 centers (Netherlands, UK, Ireland).
Patients in UC remission randomized to:
✅ Appendicectomy + standard medical therapy
vs
🧪 Standard medical therapy alone
The #ACCURE trial says: Yes. 🧵
✂️ Pragmatic, open-label RCT across 22 centers (Netherlands, UK, Ireland).
Patients in UC remission randomized to:
✅ Appendicectomy + standard medical therapy
vs
🧪 Standard medical therapy alone

Real-world 12 month outcomes of anti-TNF vs UST vs VDZ in ulcerative colitis.
UST group has 90% who are bio-experienced compared to VDZ and anti-TNF group (30+%), leading to:
1. High 'persistence' cos lack of options
2. 'Lower' efficacy of UST
#IBDSky #GISky
academic.oup.com/ecco-jcc/adv...
UST group has 90% who are bio-experienced compared to VDZ and anti-TNF group (30+%), leading to:
1. High 'persistence' cos lack of options
2. 'Lower' efficacy of UST
#IBDSky #GISky
academic.oup.com/ecco-jcc/adv...



March 30, 2025 at 12:57 AM
Real-world 12 month outcomes of anti-TNF vs UST vs VDZ in ulcerative colitis.
UST group has 90% who are bio-experienced compared to VDZ and anti-TNF group (30+%), leading to:
1. High 'persistence' cos lack of options
2. 'Lower' efficacy of UST
#IBDSky #GISky
academic.oup.com/ecco-jcc/adv...
UST group has 90% who are bio-experienced compared to VDZ and anti-TNF group (30+%), leading to:
1. High 'persistence' cos lack of options
2. 'Lower' efficacy of UST
#IBDSky #GISky
academic.oup.com/ecco-jcc/adv...
Colorectal cancer screening:
- FIT is non-inferior to colonoscopy for CRC-related deaths at 10 years
n= 57404
Participation rates higher for FIT (39.9%) vs scope (31.8%)
CRC-deaths similar: FIT (0.24%) vs scope (0.22%)
#GISky #SurgSky
@thelancet.bsky.social
www.thelancet.com/journals/lan...
- FIT is non-inferior to colonoscopy for CRC-related deaths at 10 years
n= 57404
Participation rates higher for FIT (39.9%) vs scope (31.8%)
CRC-deaths similar: FIT (0.24%) vs scope (0.22%)
#GISky #SurgSky
@thelancet.bsky.social
www.thelancet.com/journals/lan...




March 29, 2025 at 7:28 AM
Colorectal cancer screening:
- FIT is non-inferior to colonoscopy for CRC-related deaths at 10 years
n= 57404
Participation rates higher for FIT (39.9%) vs scope (31.8%)
CRC-deaths similar: FIT (0.24%) vs scope (0.22%)
#GISky #SurgSky
@thelancet.bsky.social
www.thelancet.com/journals/lan...
- FIT is non-inferior to colonoscopy for CRC-related deaths at 10 years
n= 57404
Participation rates higher for FIT (39.9%) vs scope (31.8%)
CRC-deaths similar: FIT (0.24%) vs scope (0.22%)
#GISky #SurgSky
@thelancet.bsky.social
www.thelancet.com/journals/lan...
Primary Sclerosing Cholangitis
- higher risk of colorectal Ca, biliary Ca and cirrhosis
- dx: MRC, histology, ALP/GGT, IBD
- no proven therapy, UDCA can be considered for high-risk patients
#LiverSky #GISky
www.nature.com/articles/s41...
- higher risk of colorectal Ca, biliary Ca and cirrhosis
- dx: MRC, histology, ALP/GGT, IBD
- no proven therapy, UDCA can be considered for high-risk patients
#LiverSky #GISky
www.nature.com/articles/s41...




March 23, 2025 at 1:00 AM
Primary Sclerosing Cholangitis
- higher risk of colorectal Ca, biliary Ca and cirrhosis
- dx: MRC, histology, ALP/GGT, IBD
- no proven therapy, UDCA can be considered for high-risk patients
#LiverSky #GISky
www.nature.com/articles/s41...
- higher risk of colorectal Ca, biliary Ca and cirrhosis
- dx: MRC, histology, ALP/GGT, IBD
- no proven therapy, UDCA can be considered for high-risk patients
#LiverSky #GISky
www.nature.com/articles/s41...
Granuloma in histology: Tuberculosis vs Crohn's?
TB:
- necrotizing (caseating), >400 microns, multiple (>5/hpf), submucosa, confluent
Crohn's:
- non-necrotizing, <200 microns, infrequent, mucosa, non-confluent
tl;dr: TB granulomas are larger, 'deeper' and more extensive.
#IBDSky #GISky #IDSky
TB:
- necrotizing (caseating), >400 microns, multiple (>5/hpf), submucosa, confluent
Crohn's:
- non-necrotizing, <200 microns, infrequent, mucosa, non-confluent
tl;dr: TB granulomas are larger, 'deeper' and more extensive.
#IBDSky #GISky #IDSky



February 23, 2025 at 8:55 AM
Positioning of advanced therapies in IBD, 2025
Crohn's
1st line: anti-TNF (+IM), RZK
2nd line: RZK, UPA
UC
1st line: VDZ, IFX, anti-p19
2nd line: UPA, TOFA, IFX, UST, anti-p19
@amergastroassn.bsky.social
#IBDSky #GISky
Crohn's
1st line: anti-TNF (+IM), RZK
2nd line: RZK, UPA
UC
1st line: VDZ, IFX, anti-p19
2nd line: UPA, TOFA, IFX, UST, anti-p19
@amergastroassn.bsky.social
#IBDSky #GISky



February 16, 2025 at 3:20 AM
Positioning of advanced therapies in IBD, 2025
Crohn's
1st line: anti-TNF (+IM), RZK
2nd line: RZK, UPA
UC
1st line: VDZ, IFX, anti-p19
2nd line: UPA, TOFA, IFX, UST, anti-p19
@amergastroassn.bsky.social
#IBDSky #GISky
Crohn's
1st line: anti-TNF (+IM), RZK
2nd line: RZK, UPA
UC
1st line: VDZ, IFX, anti-p19
2nd line: UPA, TOFA, IFX, UST, anti-p19
@amergastroassn.bsky.social
#IBDSky #GISky
Defunctioning stomas are used to treat refractory Crohn's disease
- most are permanent (low rates of successful reversal)
- some go on to have proctectomy for perianal disease
- successful reversal is a/w anti-TNF treatment
#IBDSky #SurgSky
pubmed.ncbi.nlm.nih.gov/39887905/
- most are permanent (low rates of successful reversal)
- some go on to have proctectomy for perianal disease
- successful reversal is a/w anti-TNF treatment
#IBDSky #SurgSky
pubmed.ncbi.nlm.nih.gov/39887905/



February 12, 2025 at 7:58 AM
Defunctioning stomas are used to treat refractory Crohn's disease
- most are permanent (low rates of successful reversal)
- some go on to have proctectomy for perianal disease
- successful reversal is a/w anti-TNF treatment
#IBDSky #SurgSky
pubmed.ncbi.nlm.nih.gov/39887905/
- most are permanent (low rates of successful reversal)
- some go on to have proctectomy for perianal disease
- successful reversal is a/w anti-TNF treatment
#IBDSky #SurgSky
pubmed.ncbi.nlm.nih.gov/39887905/
Useful article on how to handle IBD medications peri-operatively.
- IBD vs non-IBD surgery
- biologics vs small molecules
- risk of complications
- urgency of surgery
- post-op IBD treatment plans
#GISky #IBDSky #SurgSky
www.cghjournal.org/article/S154...
@amergastroassn.bsky.social
- IBD vs non-IBD surgery
- biologics vs small molecules
- risk of complications
- urgency of surgery
- post-op IBD treatment plans
#GISky #IBDSky #SurgSky
www.cghjournal.org/article/S154...
@amergastroassn.bsky.social




January 30, 2025 at 6:55 AM
Useful article on how to handle IBD medications peri-operatively.
- IBD vs non-IBD surgery
- biologics vs small molecules
- risk of complications
- urgency of surgery
- post-op IBD treatment plans
#GISky #IBDSky #SurgSky
www.cghjournal.org/article/S154...
@amergastroassn.bsky.social
- IBD vs non-IBD surgery
- biologics vs small molecules
- risk of complications
- urgency of surgery
- post-op IBD treatment plans
#GISky #IBDSky #SurgSky
www.cghjournal.org/article/S154...
@amergastroassn.bsky.social
Guidelines for Hepatitis B Virus reactivation
- anti-integrin and anti-cytokines classified as "high risk" (>10% HBVr in HBsAg+)
- VDZ and UST would be "high risk"
--> but VDZ classified as "gut specific anti-T cell rx"
--> did not expect UST to be "high risk"
#IBDSky #LiverSky
- anti-integrin and anti-cytokines classified as "high risk" (>10% HBVr in HBsAg+)
- VDZ and UST would be "high risk"
--> but VDZ classified as "gut specific anti-T cell rx"
--> did not expect UST to be "high risk"
#IBDSky #LiverSky




January 25, 2025 at 10:53 PM
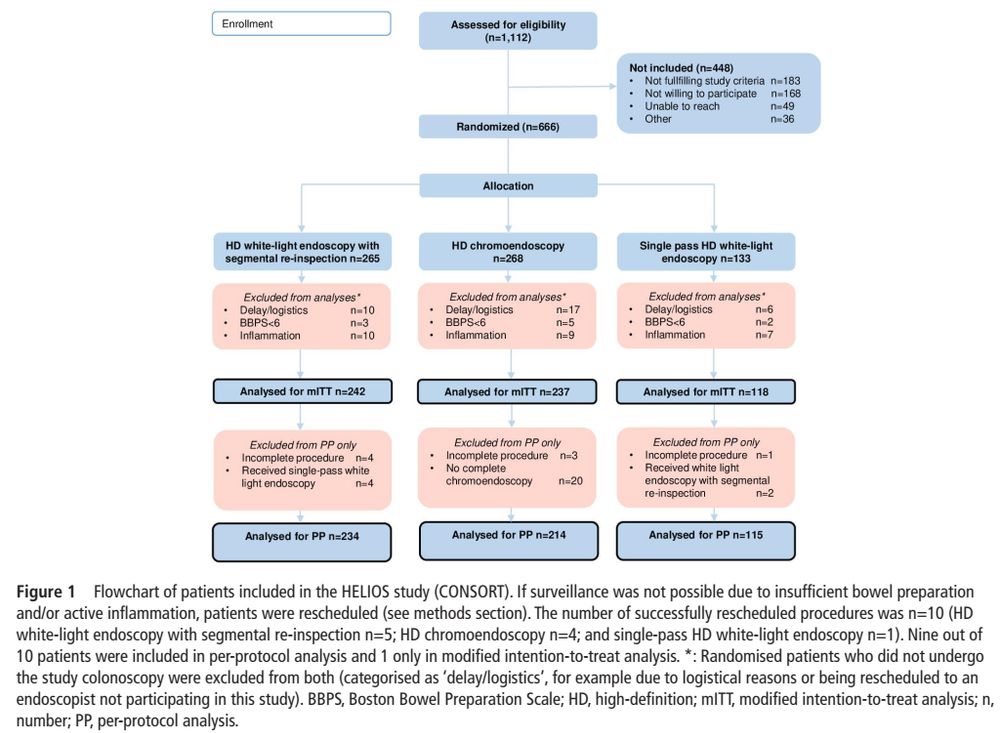
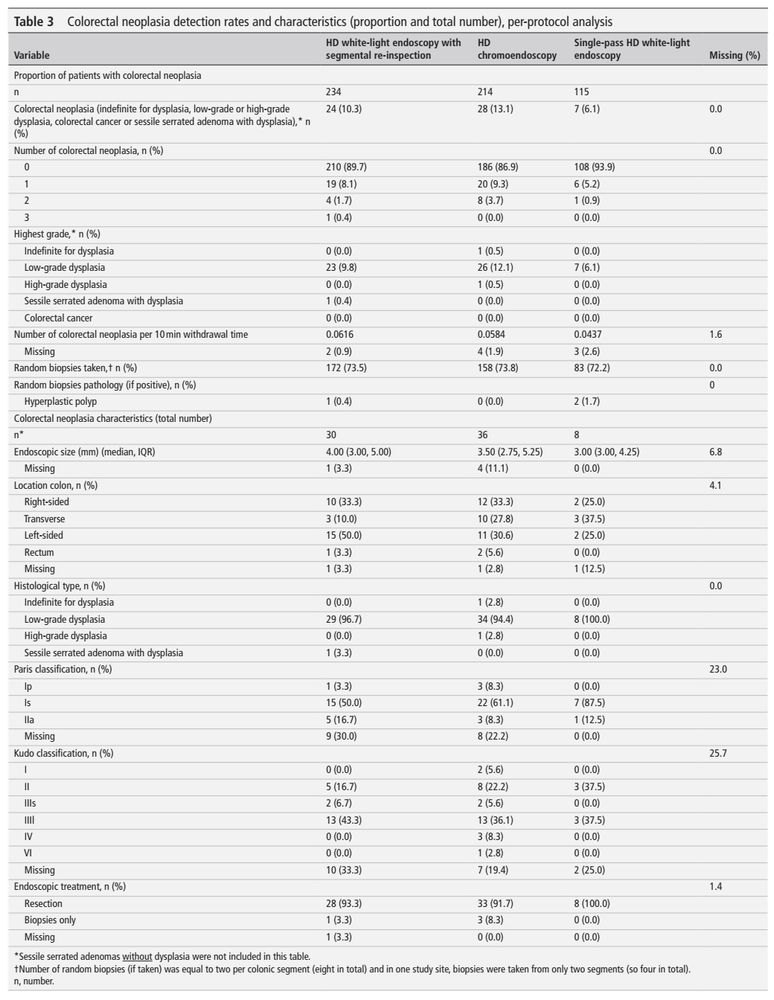
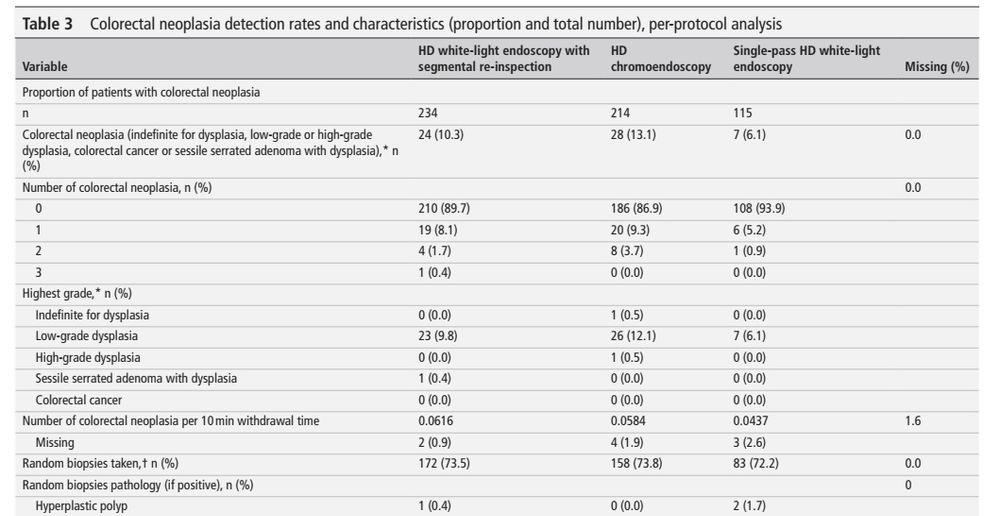
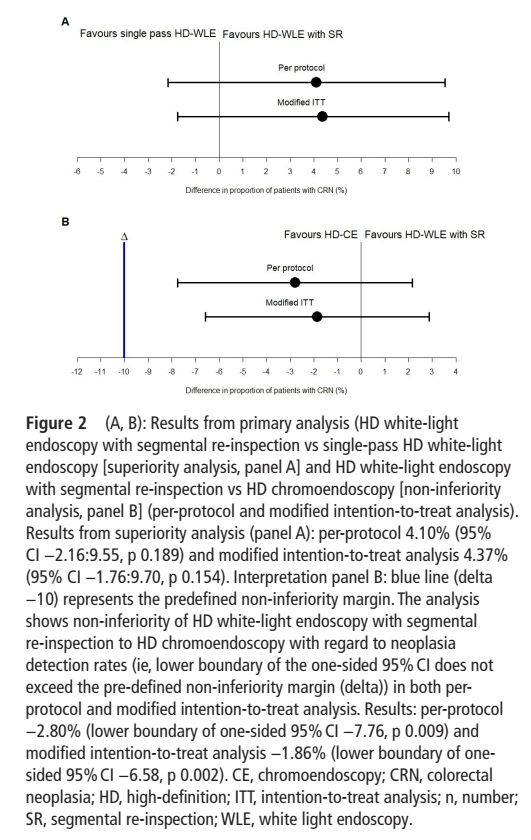
HELIOS trial (neoplasia detection in IBD)
- high-def segmental re-inspection is not inferior to high-def chromoendoscopy (10.3% vs 13.1%, non-inferiority margin of 10%)
- 'benefit' of chromoendoscopy might be due to withdrawal/inspection time
- overall neoplasia rate was low (10.5%)
#IBDSky
- high-def segmental re-inspection is not inferior to high-def chromoendoscopy (10.3% vs 13.1%, non-inferiority margin of 10%)
- 'benefit' of chromoendoscopy might be due to withdrawal/inspection time
- overall neoplasia rate was low (10.5%)
#IBDSky
January 18, 2025 at 5:41 AM
HELIOS trial (neoplasia detection in IBD)
- high-def segmental re-inspection is not inferior to high-def chromoendoscopy (10.3% vs 13.1%, non-inferiority margin of 10%)
- 'benefit' of chromoendoscopy might be due to withdrawal/inspection time
- overall neoplasia rate was low (10.5%)
#IBDSky
- high-def segmental re-inspection is not inferior to high-def chromoendoscopy (10.3% vs 13.1%, non-inferiority margin of 10%)
- 'benefit' of chromoendoscopy might be due to withdrawal/inspection time
- overall neoplasia rate was low (10.5%)
#IBDSky