


Jonathan Zuckerman MD PhD
@jzrenalpath.bsky.social
Service Chief, Renal Pathology, UCLA Department of Pathology and Laboratory Medicine. Views are my own.
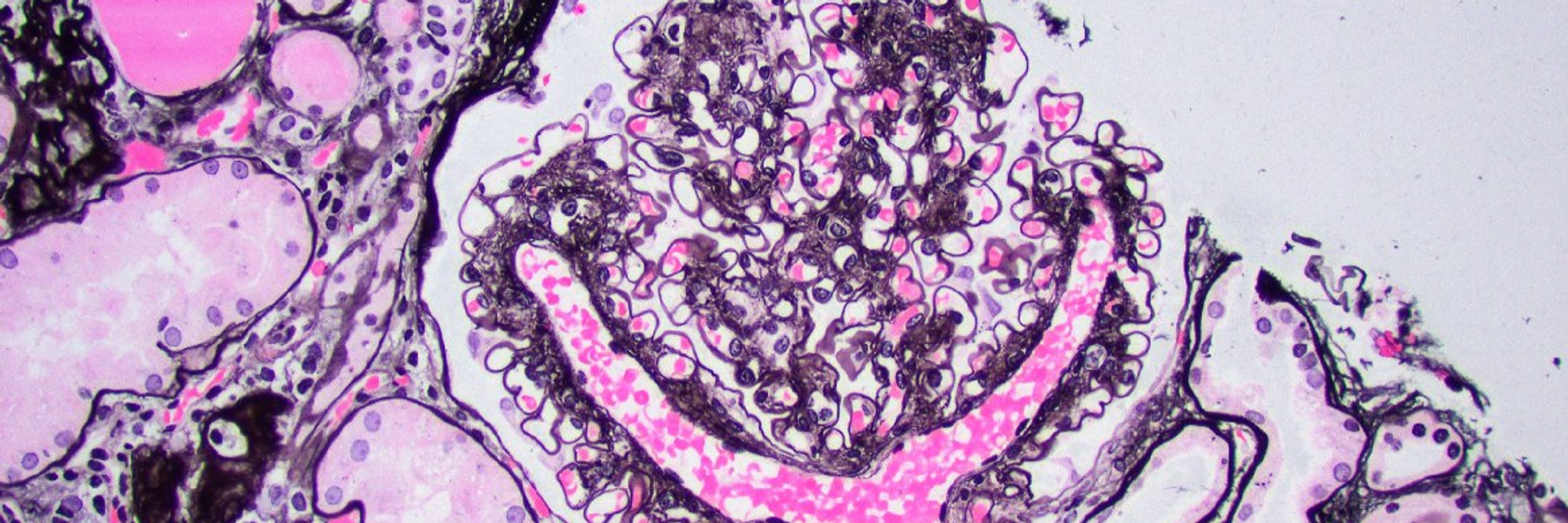
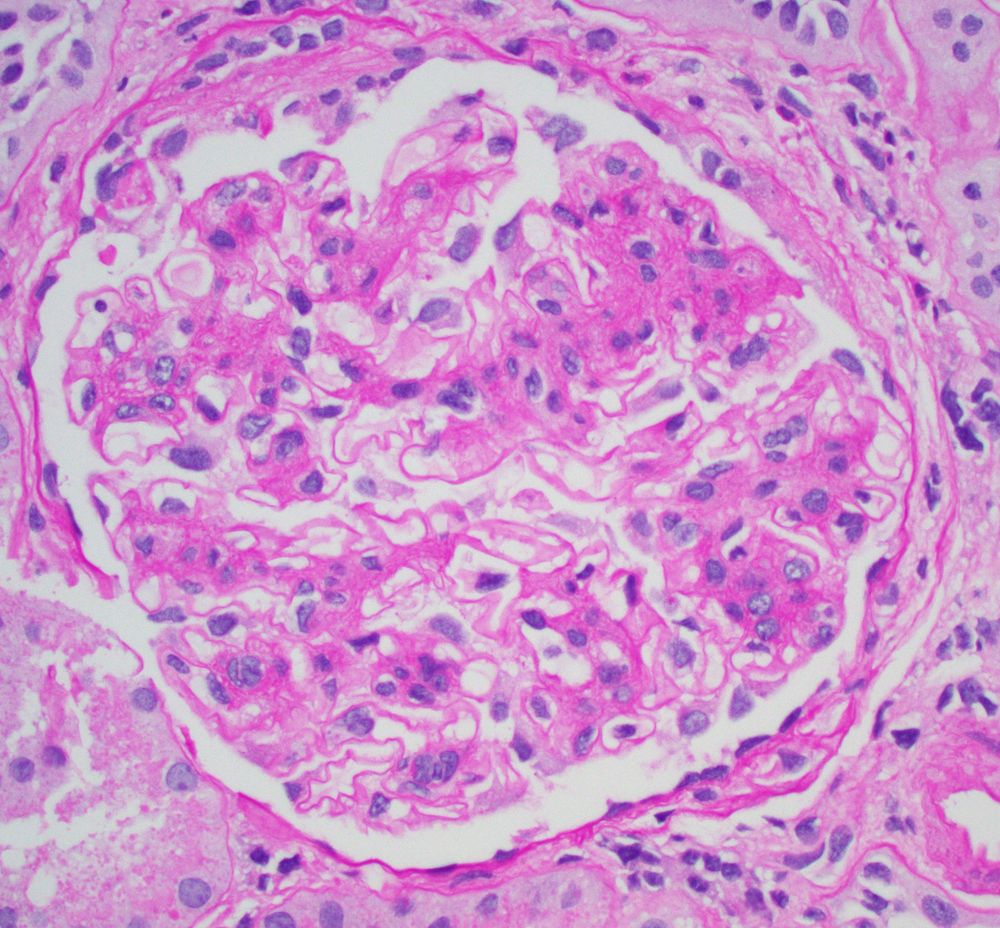
Unfortunate but not rare IgAN presentation. Pt in their 30's, no PMHx, presented with HTN emergency, CKD, hematuria, proteinuria. Advanced IgAN with severe IFTA, focal active crescents (M1 E1 S1 T2 C1). Wish we could catch these cases earlier. #renalpath #pathsky #nephsky



November 23, 2025 at 3:50 PM
Unfortunate but not rare IgAN presentation. Pt in their 30's, no PMHx, presented with HTN emergency, CKD, hematuria, proteinuria. Advanced IgAN with severe IFTA, focal active crescents (M1 E1 S1 T2 C1). Wish we could catch these cases earlier. #renalpath #pathsky #nephsky
Unusual granular casts with annular appearance. Light chain, hemoglobin, myoglobin, chromogranin casts excluded. Patient on IV vancomycin. Suspicious for vancomycin cast nephropathy. pubmed.ncbi.nlm.nih.gov/31871855/ #renalpath #pathsky #nephsky




November 21, 2025 at 3:11 PM
Unusual granular casts with annular appearance. Light chain, hemoglobin, myoglobin, chromogranin casts excluded. Patient on IV vancomycin. Suspicious for vancomycin cast nephropathy. pubmed.ncbi.nlm.nih.gov/31871855/ #renalpath #pathsky #nephsky
Reposted by Jonathan Zuckerman MD PhD

Renal hemosiderosis secondary to intravascular hemolytic anemia
doi.org/10.1016/j.kint.2025.05.033
🔹Rare case of secondary renal hemosiderosis after valve surgery
🔹Beautiful histology, Prussian blue, and EM images showing hemosiderin deposit
#MedSky #NephSky @umontreal-en.bsky.social
doi.org/10.1016/j.kint.2025.05.033
🔹Rare case of secondary renal hemosiderosis after valve surgery
🔹Beautiful histology, Prussian blue, and EM images showing hemosiderin deposit
#MedSky #NephSky @umontreal-en.bsky.social

November 20, 2025 at 7:25 PM
Renal hemosiderosis secondary to intravascular hemolytic anemia
doi.org/10.1016/j.kint.2025.05.033
🔹Rare case of secondary renal hemosiderosis after valve surgery
🔹Beautiful histology, Prussian blue, and EM images showing hemosiderin deposit
#MedSky #NephSky @umontreal-en.bsky.social
doi.org/10.1016/j.kint.2025.05.033
🔹Rare case of secondary renal hemosiderosis after valve surgery
🔹Beautiful histology, Prussian blue, and EM images showing hemosiderin deposit
#MedSky #NephSky @umontreal-en.bsky.social
Diagnosis unmasked. Young F with 2g proteinuria, weak +dsDNA. Membranous pattern, IF with C3 dominant staining. Pronase IF --> IgG-k. Membranous-like glomerulopathy with masked monotypic IgG-k deposits. Considered to be autoimmune; not MGRS. #renalpath #pathsky #nephsky.




November 20, 2025 at 1:01 PM
Diagnosis unmasked. Young F with 2g proteinuria, weak +dsDNA. Membranous pattern, IF with C3 dominant staining. Pronase IF --> IgG-k. Membranous-like glomerulopathy with masked monotypic IgG-k deposits. Considered to be autoimmune; not MGRS. #renalpath #pathsky #nephsky.
BK nephropathy
Clues:
- Heavy but focal tubulointerstitial inflammation
- Increased plasma cells
- Viral cytopathic change
- Features of CNI toxicity ->over immunosuppression (isometric vacuolization shown here)
-SV40 IHC confirmatory
#renalpath #pathsky #nephsky
Clues:
- Heavy but focal tubulointerstitial inflammation
- Increased plasma cells
- Viral cytopathic change
- Features of CNI toxicity ->over immunosuppression (isometric vacuolization shown here)
-SV40 IHC confirmatory
#renalpath #pathsky #nephsky




November 19, 2025 at 3:35 PM
BK nephropathy
Clues:
- Heavy but focal tubulointerstitial inflammation
- Increased plasma cells
- Viral cytopathic change
- Features of CNI toxicity ->over immunosuppression (isometric vacuolization shown here)
-SV40 IHC confirmatory
#renalpath #pathsky #nephsky
Clues:
- Heavy but focal tubulointerstitial inflammation
- Increased plasma cells
- Viral cytopathic change
- Features of CNI toxicity ->over immunosuppression (isometric vacuolization shown here)
-SV40 IHC confirmatory
#renalpath #pathsky #nephsky
Arteriole with features of a old recanalized thombus in a transplant kidney biopsy. Multiple slit like vascular spaces within the fibrotic lumen. Not a lesion I see often. Pt had clinically diagnosed TMA a few months prior. #renalpath #pathsky #nephsky

November 18, 2025 at 6:29 PM
Arteriole with features of a old recanalized thombus in a transplant kidney biopsy. Multiple slit like vascular spaces within the fibrotic lumen. Not a lesion I see often. Pt had clinically diagnosed TMA a few months prior. #renalpath #pathsky #nephsky
Reposted by Jonathan Zuckerman MD PhD
Chronic active ABMR in patient with worsening proteinuria, renal function, positive DSA
*Glomerulitis (shown in image)
*Transplant glomerulopathy (shown in image)
*Peritubular capillaritis
*Diffuse C4d+ in PTCs on IF
#renalpath #transplant #pathsky #nephsky #medsky
*Glomerulitis (shown in image)
*Transplant glomerulopathy (shown in image)
*Peritubular capillaritis
*Diffuse C4d+ in PTCs on IF
#renalpath #transplant #pathsky #nephsky #medsky

April 7, 2025 at 3:50 AM
Chronic active ABMR in patient with worsening proteinuria, renal function, positive DSA
*Glomerulitis (shown in image)
*Transplant glomerulopathy (shown in image)
*Peritubular capillaritis
*Diffuse C4d+ in PTCs on IF
#renalpath #transplant #pathsky #nephsky #medsky
*Glomerulitis (shown in image)
*Transplant glomerulopathy (shown in image)
*Peritubular capillaritis
*Diffuse C4d+ in PTCs on IF
#renalpath #transplant #pathsky #nephsky #medsky
NELL-1 IHC can also be tricky to interpret as there is significant podocyte cytoplasmic staining in the negative control. Must show granular capillary wall deposits which match deposits by IF and EM. #renalpath #pathsky #nephsky

November 17, 2025 at 8:06 PM
NELL-1 IHC can also be tricky to interpret as there is significant podocyte cytoplasmic staining in the negative control. Must show granular capillary wall deposits which match deposits by IF and EM. #renalpath #pathsky #nephsky
Illustrative example of a segmental membranous nephropathy pattern (segmental granular IgG staining) which is often seen with NELL-1+ (IHC) MN as in this case. Deposits present in only some loops by EM. #renalpath #pathsky #nephsky




November 17, 2025 at 8:03 PM
Illustrative example of a segmental membranous nephropathy pattern (segmental granular IgG staining) which is often seen with NELL-1+ (IHC) MN as in this case. Deposits present in only some loops by EM. #renalpath #pathsky #nephsky
Intimate contact between endothelial cell and mesangial cell cytoplasm. A reminder that no GBM separates the blood space from the mesangium. I wonder what secrets they are sharing. #renalpath #pathsky #nephsky


October 31, 2025 at 5:09 PM
Intimate contact between endothelial cell and mesangial cell cytoplasm. A reminder that no GBM separates the blood space from the mesangium. I wonder what secrets they are sharing. #renalpath #pathsky #nephsky
Severe vascular rejection hiding in the IF tissue. Fibrinoid necrosis really pops on the H&E and further confirmed by fibrinogen IF. #renalpath #pathsky #nephsky


October 31, 2025 at 5:04 PM
Severe vascular rejection hiding in the IF tissue. Fibrinoid necrosis really pops on the H&E and further confirmed by fibrinogen IF. #renalpath #pathsky #nephsky
Reposted by Jonathan Zuckerman MD PhD

Laser microdissection followed by mass spectrometry (LMD/MS) shows promise as a more sensitive approach to tissue diagnosis of PLA2R-associated membranous nephropathy. Read more in #ASNKidneyNews kidney.pub/KN1710-09

October 27, 2025 at 2:00 PM
Laser microdissection followed by mass spectrometry (LMD/MS) shows promise as a more sensitive approach to tissue diagnosis of PLA2R-associated membranous nephropathy. Read more in #ASNKidneyNews kidney.pub/KN1710-09
Reposted by Jonathan Zuckerman MD PhD

📽️✨An inside look at life in the UCLA Pathology Residency Program!
We’re excited to share the moments that shape our residents -
from the microscope to mentorship, and everything in between.
Watch the full video ➨ youtu.be/Yfw39_U9_Hg
#pathology #PathSky #PathMatch26 #PathMatch #Match2026
We’re excited to share the moments that shape our residents -
from the microscope to mentorship, and everything in between.
Watch the full video ➨ youtu.be/Yfw39_U9_Hg
#pathology #PathSky #PathMatch26 #PathMatch #Match2026

UCLA Pathology & Laboratory Medicine Residency Program
YouTube video by UCLA Department of Pathology & Laboratory Medicine
youtu.be
October 22, 2025 at 4:00 PM
📽️✨An inside look at life in the UCLA Pathology Residency Program!
We’re excited to share the moments that shape our residents -
from the microscope to mentorship, and everything in between.
Watch the full video ➨ youtu.be/Yfw39_U9_Hg
#pathology #PathSky #PathMatch26 #PathMatch #Match2026
We’re excited to share the moments that shape our residents -
from the microscope to mentorship, and everything in between.
Watch the full video ➨ youtu.be/Yfw39_U9_Hg
#pathology #PathSky #PathMatch26 #PathMatch #Match2026
Teenager with nephrotic syndrome. Biopsy revealed unusual case of membranous nephropathy in a peds patient. PLA2R positive (IHC). PLA2R most common antigen in peds MN. EXT1/2 also common, SEMA3B less common. (pubmed.ncbi.nlm.nih.gov/38025223/) #renalpath #pathsky #nephsky




October 13, 2025 at 1:56 PM
Teenager with nephrotic syndrome. Biopsy revealed unusual case of membranous nephropathy in a peds patient. PLA2R positive (IHC). PLA2R most common antigen in peds MN. EXT1/2 also common, SEMA3B less common. (pubmed.ncbi.nlm.nih.gov/38025223/) #renalpath #pathsky #nephsky
A startling biopsy. Severe acute TMA in a pt with suspected scleroderma renal crisis. Massive vascular thrombosis, mucoid intimal edema, and early onion skin change associated with severe cortical necrosis. #renalpath #nephsky #pathsky




October 9, 2025 at 3:08 AM
A startling biopsy. Severe acute TMA in a pt with suspected scleroderma renal crisis. Massive vascular thrombosis, mucoid intimal edema, and early onion skin change associated with severe cortical necrosis. #renalpath #nephsky #pathsky
Bx for nephrotic syndrome in an IV drug user with multiple infections. LM was all medulla, but good enough to make a diagnosis. AA amyloidosis; very common bx result in this clinical setting. #renalpath #pathsky #nephsky



October 7, 2025 at 5:32 PM
Bx for nephrotic syndrome in an IV drug user with multiple infections. LM was all medulla, but good enough to make a diagnosis. AA amyloidosis; very common bx result in this clinical setting. #renalpath #pathsky #nephsky
Bx for new onset NS in an older adult. Serologic work up including SPEP/UPEP IFE negative. Bx shows membranous pattern with few double contours. IgG3-k restriction and mottle EM deposits c/w PGNMID with membranous predominant pattern. PLA2R- #renalpath #pathsky #nephsky


October 5, 2025 at 3:30 PM
Bx for new onset NS in an older adult. Serologic work up including SPEP/UPEP IFE negative. Bx shows membranous pattern with few double contours. IgG3-k restriction and mottle EM deposits c/w PGNMID with membranous predominant pattern. PLA2R- #renalpath #pathsky #nephsky
Kidney txp biopsy for AKI (~6 post txp). Tubular injury associated with granular and ropey trichome positive casts. IHC confirmed myoglobin cast nephropathy. CK found to be very high; thought to be due to statin related myopathy. #renalpath #pathsky #nephsky



October 4, 2025 at 5:17 PM
Kidney txp biopsy for AKI (~6 post txp). Tubular injury associated with granular and ropey trichome positive casts. IHC confirmed myoglobin cast nephropathy. CK found to be very high; thought to be due to statin related myopathy. #renalpath #pathsky #nephsky
Heavy Chains, Heavy Consequences: A Case of Concomitant Heavy Chain Amyloidosis and Heavy Chain Deposition Disease. Fibrils and powdery deposits. #renalpath #nephsky #pathsky www.sciencedirect.com/science/arti...


September 17, 2025 at 6:13 PM
Heavy Chains, Heavy Consequences: A Case of Concomitant Heavy Chain Amyloidosis and Heavy Chain Deposition Disease. Fibrils and powdery deposits. #renalpath #nephsky #pathsky www.sciencedirect.com/science/arti...
Reposted by Jonathan Zuckerman MD PhD
🔬 We are now recruiting a Renal Pathologist! #pathology #path2path #PathSky #renalpath
Join our team today! ➨ bit.ly/46CqsrU
Join our team today! ➨ bit.ly/46CqsrU
September 17, 2025 at 4:33 PM
🔬 We are now recruiting a Renal Pathologist! #pathology #path2path #PathSky #renalpath
Join our team today! ➨ bit.ly/46CqsrU
Join our team today! ➨ bit.ly/46CqsrU
Multiple diagnoses not uncommon in kidney biopsies. This case showed nodular diabetic nephropathy, a mostly chronic ANCA associated GN, and to top it off some interstitial ALECT2 amyloidosis. #renalpath #nephsky #pathsky




September 11, 2025 at 5:21 PM
Multiple diagnoses not uncommon in kidney biopsies. This case showed nodular diabetic nephropathy, a mostly chronic ANCA associated GN, and to top it off some interstitial ALECT2 amyloidosis. #renalpath #nephsky #pathsky
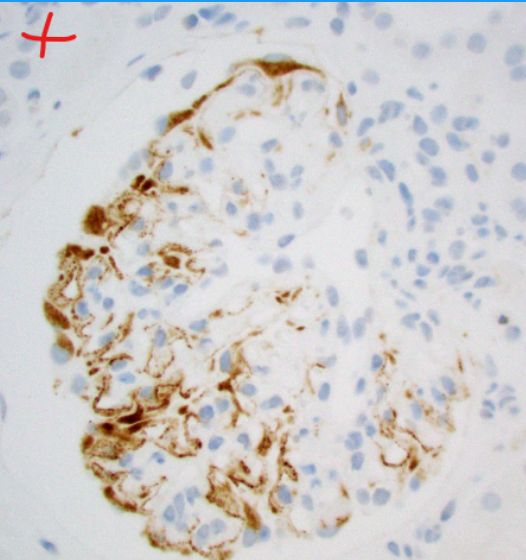
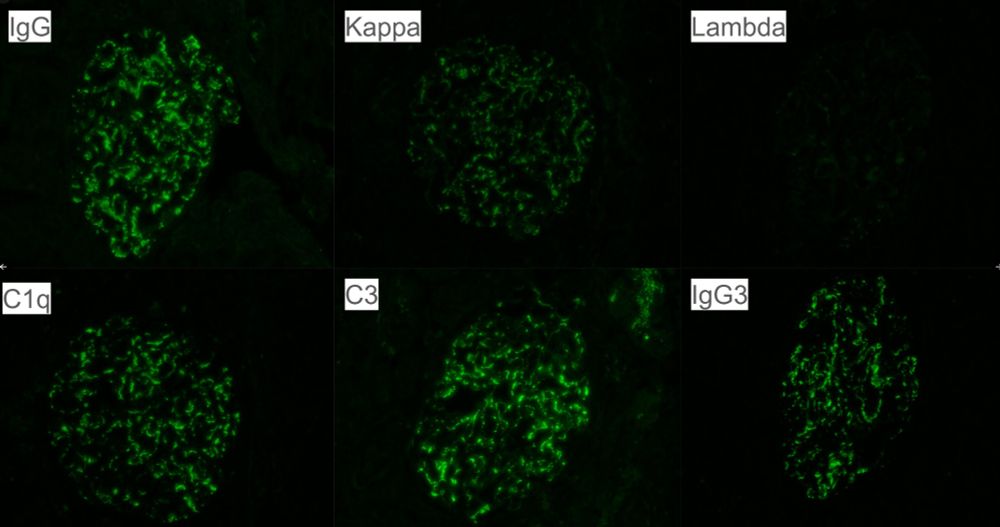
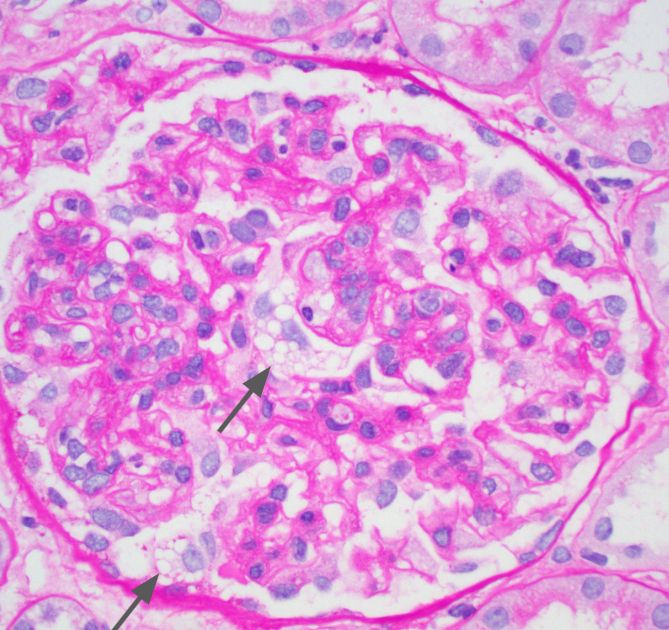
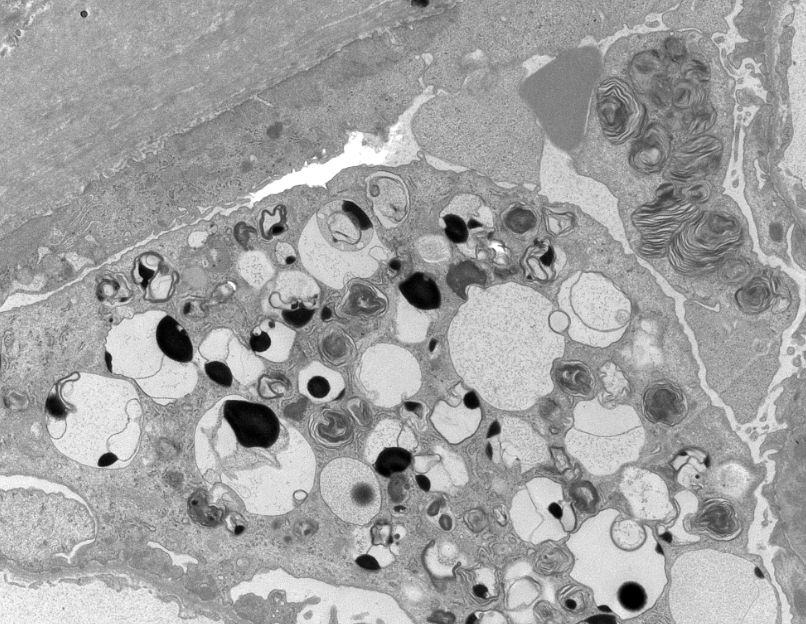
Lupus nephritis case with prominent podocyte cytoplasmic vacuolization on LM with myelin figures revealed by EM. Probably HCQ effect but given its prominence genetic etiologies should be excluded (e.g., Fabry, LMX1B). #renalpath #pathsky #nephsky


September 8, 2025 at 11:06 PM
Lupus nephritis case with prominent podocyte cytoplasmic vacuolization on LM with myelin figures revealed by EM. Probably HCQ effect but given its prominence genetic etiologies should be excluded (e.g., Fabry, LMX1B). #renalpath #pathsky #nephsky
Interesting case of AL-amyloidosis. Massive vascular deposits, even in hilar arterioles with glomerular sparring. Patient had minimal proteinuria given lack of glomerular amyloid. #renalpath #pathsky #nephsky




September 4, 2025 at 11:14 PM
Interesting case of AL-amyloidosis. Massive vascular deposits, even in hilar arterioles with glomerular sparring. Patient had minimal proteinuria given lack of glomerular amyloid. #renalpath #pathsky #nephsky
Nice example of urate crystals in gouty tophi involving the medulla. Polarizable crystals can be see using unstained sections from the IF tissue. #renalpath #pathsky #nephsky


August 28, 2025 at 7:04 PM
Nice example of urate crystals in gouty tophi involving the medulla. Polarizable crystals can be see using unstained sections from the IF tissue. #renalpath #pathsky #nephsky
Another example of an 'incidental' finding next to the tumor in a nephrectomy specimen. Amyloidosis (probably LECT2). Reminder not too overlook the non-neoplastic tissue. #renalpath #pathsky #nephsky



August 20, 2025 at 4:55 PM
Another example of an 'incidental' finding next to the tumor in a nephrectomy specimen. Amyloidosis (probably LECT2). Reminder not too overlook the non-neoplastic tissue. #renalpath #pathsky #nephsky