



Filippo D’Amico
@filippodamico.bsky.social
Anesthesia and Intensive care San Raffaele Hospital
#ISICEM25 | Cardiac-Synchronized Mechanical Ventilation? 🫁❤️
🔬 Markus Skrifvars explores its impact:
✅ Higher PaO₂ & lower PaCO₂ with no pressure differences
❓ Key question: Are pneumothorax findings relevant to humans, or is this an effect seen only in pigs? 🐷
🔬 Markus Skrifvars explores its impact:
✅ Higher PaO₂ & lower PaCO₂ with no pressure differences
❓ Key question: Are pneumothorax findings relevant to humans, or is this an effect seen only in pigs? 🐷

March 21, 2025 at 2:16 PM
#ISICEM25 | Cardiac-Synchronized Mechanical Ventilation? 🫁❤️
🔬 Markus Skrifvars explores its impact:
✅ Higher PaO₂ & lower PaCO₂ with no pressure differences
❓ Key question: Are pneumothorax findings relevant to humans, or is this an effect seen only in pigs? 🐷
🔬 Markus Skrifvars explores its impact:
✅ Higher PaO₂ & lower PaCO₂ with no pressure differences
❓ Key question: Are pneumothorax findings relevant to humans, or is this an effect seen only in pigs? 🐷
#ISICEM25 | Key Questions in Advanced Airway Management 🫁❓
🔥 Ari Moskowitz highlights ongoing debates:
🔹 Best device? ETI vs. SGA 🤔
🔹 Video vs. Direct Laryngoscopy 📹
🔹 When to intubate? Timing remains unclear ⏳
🔹 Should strategy vary based on arrest etiology, rhythm, or location?
🔥 Ari Moskowitz highlights ongoing debates:
🔹 Best device? ETI vs. SGA 🤔
🔹 Video vs. Direct Laryngoscopy 📹
🔹 When to intubate? Timing remains unclear ⏳
🔹 Should strategy vary based on arrest etiology, rhythm, or location?


March 21, 2025 at 2:15 PM
#ISICEM25 | Key Questions in Advanced Airway Management 🫁❓
🔥 Ari Moskowitz highlights ongoing debates:
🔹 Best device? ETI vs. SGA 🤔
🔹 Video vs. Direct Laryngoscopy 📹
🔹 When to intubate? Timing remains unclear ⏳
🔹 Should strategy vary based on arrest etiology, rhythm, or location?
🔥 Ari Moskowitz highlights ongoing debates:
🔹 Best device? ETI vs. SGA 🤔
🔹 Video vs. Direct Laryngoscopy 📹
🔹 When to intubate? Timing remains unclear ⏳
🔹 Should strategy vary based on arrest etiology, rhythm, or location?
#ISICEM25 | Key Questions in Advanced Airway Management 🫁❓
🔥 Ari Moskowitz highlights ongoing debates:
🔹 Best device? ETI vs. SGA 🤔
🔹 Video vs. Direct Laryngoscopy 📹
🔹 When to intubate? Timing remains unclear ⏳
🔹 Should strategy vary based on arrest etiology, rhythm, or location?
🔥 Ari Moskowitz highlights ongoing debates:
🔹 Best device? ETI vs. SGA 🤔
🔹 Video vs. Direct Laryngoscopy 📹
🔹 When to intubate? Timing remains unclear ⏳
🔹 Should strategy vary based on arrest etiology, rhythm, or location?
March 21, 2025 at 2:15 PM
#ISICEM25 | Key Questions in Advanced Airway Management 🫁❓
🔥 Ari Moskowitz highlights ongoing debates:
🔹 Best device? ETI vs. SGA 🤔
🔹 Video vs. Direct Laryngoscopy 📹
🔹 When to intubate? Timing remains unclear ⏳
🔹 Should strategy vary based on arrest etiology, rhythm, or location?
🔥 Ari Moskowitz highlights ongoing debates:
🔹 Best device? ETI vs. SGA 🤔
🔹 Video vs. Direct Laryngoscopy 📹
🔹 When to intubate? Timing remains unclear ⏳
🔹 Should strategy vary based on arrest etiology, rhythm, or location?
#ISICEM25 | Ari Moskowitz on Controversies in Airway Management during CPR 🫁🚑
🔹 OHCA: RCTs suggest SGA may be as good or better than ETI, based on operator skill.
🔹 IHCA: Limited data—observational studies lean toward no intubation
🔹 Ongoing trials comparing SGA vs. ETI for IHCA.
🔹 OHCA: RCTs suggest SGA may be as good or better than ETI, based on operator skill.
🔹 IHCA: Limited data—observational studies lean toward no intubation
🔹 Ongoing trials comparing SGA vs. ETI for IHCA.

March 21, 2025 at 2:14 PM
#ISICEM25 | Ari Moskowitz on Controversies in Airway Management during CPR 🫁🚑
🔹 OHCA: RCTs suggest SGA may be as good or better than ETI, based on operator skill.
🔹 IHCA: Limited data—observational studies lean toward no intubation
🔹 Ongoing trials comparing SGA vs. ETI for IHCA.
🔹 OHCA: RCTs suggest SGA may be as good or better than ETI, based on operator skill.
🔹 IHCA: Limited data—observational studies lean toward no intubation
🔹 Ongoing trials comparing SGA vs. ETI for IHCA.
#ISICEM25 | IV vs. IO Access—Key Takeaways 💉🦴
📢 Markus Skrifvars on why IV remains the first choice:
✅ Higher ROSC rate
✅ Standard method for non-cardiac arrest patients
✅ As fast as IO in most cases
✅ Less expensive
📢 Markus Skrifvars on why IV remains the first choice:
✅ Higher ROSC rate
✅ Standard method for non-cardiac arrest patients
✅ As fast as IO in most cases
✅ Less expensive

March 21, 2025 at 2:13 PM
#ISICEM25 | IV vs. IO Access—Key Takeaways 💉🦴
📢 Markus Skrifvars on why IV remains the first choice:
✅ Higher ROSC rate
✅ Standard method for non-cardiac arrest patients
✅ As fast as IO in most cases
✅ Less expensive
📢 Markus Skrifvars on why IV remains the first choice:
✅ Higher ROSC rate
✅ Standard method for non-cardiac arrest patients
✅ As fast as IO in most cases
✅ Less expensive
#ISICEM25 | IV vs. IO Access—What’s the Best Choice? 💉🦴
🔍 Markus Skrifvars explores the pros & cons:
✅ IO is as good as IV—but not better
💰 More expensive & should be second choice after IV
🚑 Useful in EMS for patients with difficult access (e.g., children)
⚡ No faster than IV
🔍 Markus Skrifvars explores the pros & cons:
✅ IO is as good as IV—but not better
💰 More expensive & should be second choice after IV
🚑 Useful in EMS for patients with difficult access (e.g., children)
⚡ No faster than IV

March 21, 2025 at 2:12 PM
#ISICEM25 | IV vs. IO Access—What’s the Best Choice? 💉🦴
🔍 Markus Skrifvars explores the pros & cons:
✅ IO is as good as IV—but not better
💰 More expensive & should be second choice after IV
🚑 Useful in EMS for patients with difficult access (e.g., children)
⚡ No faster than IV
🔍 Markus Skrifvars explores the pros & cons:
✅ IO is as good as IV—but not better
💰 More expensive & should be second choice after IV
🚑 Useful in EMS for patients with difficult access (e.g., children)
⚡ No faster than IV
#ISICEM25 | 🏥 New Guidelines for Perioperative Cardiac Arrest 🔄❤️
📢 Sharon Einav presents the methodology & PICO questions shaping the upcoming recommendations.
🔹 Evidence-based updates coming in the next few months!
🔹 Focus on best practices for managing cardiac arrest in surgical patients.
📢 Sharon Einav presents the methodology & PICO questions shaping the upcoming recommendations.
🔹 Evidence-based updates coming in the next few months!
🔹 Focus on best practices for managing cardiac arrest in surgical patients.

March 21, 2025 at 2:12 PM
#ISICEM25 | 🏥 New Guidelines for Perioperative Cardiac Arrest 🔄❤️
📢 Sharon Einav presents the methodology & PICO questions shaping the upcoming recommendations.
🔹 Evidence-based updates coming in the next few months!
🔹 Focus on best practices for managing cardiac arrest in surgical patients.
📢 Sharon Einav presents the methodology & PICO questions shaping the upcoming recommendations.
🔹 Evidence-based updates coming in the next few months!
🔹 Focus on best practices for managing cardiac arrest in surgical patients.
#ISICEM25 | 🚑 CPR Session Starting Now! 🚑
Moderated by Michel Slama & @fabio_taccone, this session dives into the latest advances in cardiopulmonary resuscitation
Moderated by Michel Slama & @fabio_taccone, this session dives into the latest advances in cardiopulmonary resuscitation

March 21, 2025 at 12:55 PM
#ISICEM25 | 🚑 CPR Session Starting Now! 🚑
Moderated by Michel Slama & @fabio_taccone, this session dives into the latest advances in cardiopulmonary resuscitation
Moderated by Michel Slama & @fabio_taccone, this session dives into the latest advances in cardiopulmonary resuscitation
#ISICEM25 | 🏆 POSTER AWARDS 2025 🏆
👏 Xavier Monnet presents this year’s best research contributions!
📊 431 abstracts submitted
✅ 321 abstracts accepted
🏅 4 awards + 1 ISF (International Sepsis Forum) award
A celebration of innovation and excellence in intensive care research!
👏 Xavier Monnet presents this year’s best research contributions!
📊 431 abstracts submitted
✅ 321 abstracts accepted
🏅 4 awards + 1 ISF (International Sepsis Forum) award
A celebration of innovation and excellence in intensive care research!

March 21, 2025 at 10:07 AM
#ISICEM25 | 🏆 POSTER AWARDS 2025 🏆
👏 Xavier Monnet presents this year’s best research contributions!
📊 431 abstracts submitted
✅ 321 abstracts accepted
🏅 4 awards + 1 ISF (International Sepsis Forum) award
A celebration of innovation and excellence in intensive care research!
👏 Xavier Monnet presents this year’s best research contributions!
📊 431 abstracts submitted
✅ 321 abstracts accepted
🏅 4 awards + 1 ISF (International Sepsis Forum) award
A celebration of innovation and excellence in intensive care research!
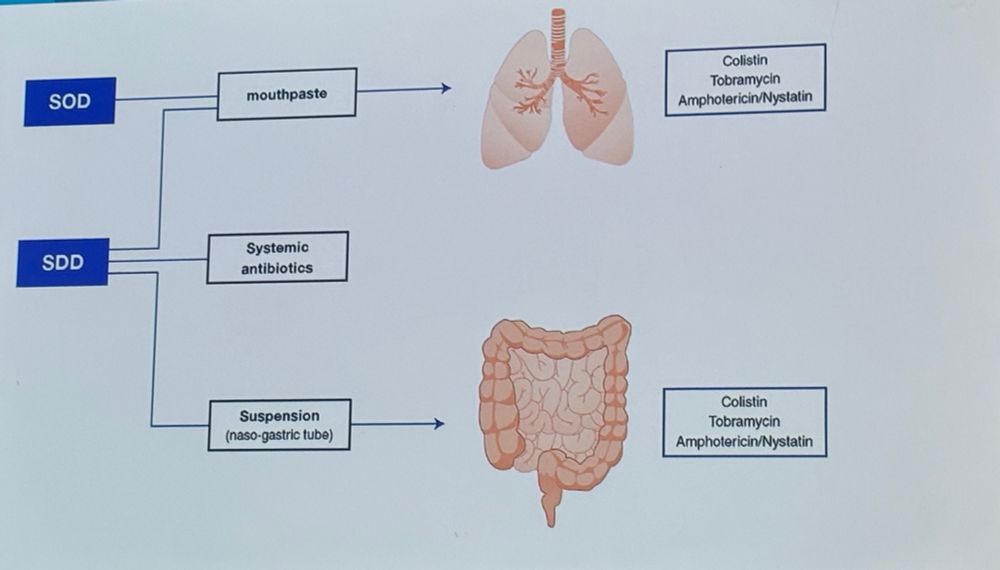
#ISICEM25 | Lennie Derde asks: Why is nobody using SDD despite strong evidence? 🤔💊
📊 Thousands of patients, consistent data, and mortality reduction, yet SDD remains underutilized.
🔹 Open questions:
•Availability
•Optimal regimen
•Impact on microbiome
📊 Thousands of patients, consistent data, and mortality reduction, yet SDD remains underutilized.
🔹 Open questions:
•Availability
•Optimal regimen
•Impact on microbiome
March 21, 2025 at 10:07 AM
#ISICEM25 | Lennie Derde asks: Why is nobody using SDD despite strong evidence? 🤔💊
📊 Thousands of patients, consistent data, and mortality reduction, yet SDD remains underutilized.
🔹 Open questions:
•Availability
•Optimal regimen
•Impact on microbiome
📊 Thousands of patients, consistent data, and mortality reduction, yet SDD remains underutilized.
🔹 Open questions:
•Availability
•Optimal regimen
•Impact on microbiome
#ISICEM25 | Paul Elbers on when to stop antibiotics—insights from data science 🔬💊
🔹 19% of patients had antibiotics reinitiated frequently
Reinitiating antibiotics is linked to:
📈 Longer ICU stay (22.0 vs. 15.9 days)
⚠️ Higher 90-day mortality (40% vs. 25%)
🔹 19% of patients had antibiotics reinitiated frequently
Reinitiating antibiotics is linked to:
📈 Longer ICU stay (22.0 vs. 15.9 days)
⚠️ Higher 90-day mortality (40% vs. 25%)

March 21, 2025 at 10:06 AM
#ISICEM25 | Paul Elbers on when to stop antibiotics—insights from data science 🔬💊
🔹 19% of patients had antibiotics reinitiated frequently
Reinitiating antibiotics is linked to:
📈 Longer ICU stay (22.0 vs. 15.9 days)
⚠️ Higher 90-day mortality (40% vs. 25%)
🔹 19% of patients had antibiotics reinitiated frequently
Reinitiating antibiotics is linked to:
📈 Longer ICU stay (22.0 vs. 15.9 days)
⚠️ Higher 90-day mortality (40% vs. 25%)
#ISICEM25 | Antoni Torres on when to stop antibiotics in severe CAP 🦠💊
🔹 Outpatients: ≤5 days if stable
🔹 Non-severe inpatients: <5 days (minimum 3)
🔹 Severe CAP: ≥5 days if stable
Key question: Can clinical stability criteria from CAP be applied to SCAP patients on mechanical ventilation?
🔹 Outpatients: ≤5 days if stable
🔹 Non-severe inpatients: <5 days (minimum 3)
🔹 Severe CAP: ≥5 days if stable
Key question: Can clinical stability criteria from CAP be applied to SCAP patients on mechanical ventilation?
March 21, 2025 at 10:05 AM
#ISICEM25 | Antoni Torres on when to stop antibiotics in severe CAP 🦠💊
🔹 Outpatients: ≤5 days if stable
🔹 Non-severe inpatients: <5 days (minimum 3)
🔹 Severe CAP: ≥5 days if stable
Key question: Can clinical stability criteria from CAP be applied to SCAP patients on mechanical ventilation?
🔹 Outpatients: ≤5 days if stable
🔹 Non-severe inpatients: <5 days (minimum 3)
🔹 Severe CAP: ≥5 days if stable
Key question: Can clinical stability criteria from CAP be applied to SCAP patients on mechanical ventilation?
#ISICEM25 | Always fascinating to hear @MichardFrederic discuss the future of bedside screens 🖥️🔍
📊 Evolution to visual decision support tools
🔹 Turning data into knowledge
⚡ Faster & more accurate detection of abnormalities
🧠 Improving situation awareness & reducing cognitive workload
📊 Evolution to visual decision support tools
🔹 Turning data into knowledge
⚡ Faster & more accurate detection of abnormalities
🧠 Improving situation awareness & reducing cognitive workload

March 20, 2025 at 5:56 PM
#ISICEM25 | Always fascinating to hear @MichardFrederic discuss the future of bedside screens 🖥️🔍
📊 Evolution to visual decision support tools
🔹 Turning data into knowledge
⚡ Faster & more accurate detection of abnormalities
🧠 Improving situation awareness & reducing cognitive workload
📊 Evolution to visual decision support tools
🔹 Turning data into knowledge
⚡ Faster & more accurate detection of abnormalities
🧠 Improving situation awareness & reducing cognitive workload
#ISICEM25 | Michard Frederic on the future of bedside monitoring! 🚀📊
🔹 New ways to display monitoring variables
🔹 Advanced tools to visualize data
🔹 Seamless data integration into a single monitor
🔹 Data fusion—combining variables into one visual tool
🔹 New ways to display monitoring variables
🔹 Advanced tools to visualize data
🔹 Seamless data integration into a single monitor
🔹 Data fusion—combining variables into one visual tool

March 20, 2025 at 5:56 PM
#ISICEM25 | Michard Frederic on the future of bedside monitoring! 🚀📊
🔹 New ways to display monitoring variables
🔹 Advanced tools to visualize data
🔹 Seamless data integration into a single monitor
🔹 Data fusion—combining variables into one visual tool
🔹 New ways to display monitoring variables
🔹 Advanced tools to visualize data
🔹 Seamless data integration into a single monitor
🔹 Data fusion—combining variables into one visual tool
#ISICEM25 | Vitaly Herasevich on building smart alerts in critical care ⚡🔍
🔹 No perfect detection algorithm exists—manual confirmation is key
🔹 Visual decision support tools enhance clinician feedback
🔹 Real-time compliance reports enable reinforced learning
🔹 No perfect detection algorithm exists—manual confirmation is key
🔹 Visual decision support tools enhance clinician feedback
🔹 Real-time compliance reports enable reinforced learning


March 20, 2025 at 5:56 PM
#ISICEM25 | Vitaly Herasevich on building smart alerts in critical care ⚡🔍
🔹 No perfect detection algorithm exists—manual confirmation is key
🔹 Visual decision support tools enhance clinician feedback
🔹 Real-time compliance reports enable reinforced learning
🔹 No perfect detection algorithm exists—manual confirmation is key
🔹 Visual decision support tools enhance clinician feedback
🔹 Real-time compliance reports enable reinforced learning
#ISICEM25 | Michael R. Pinsky on Autonomous Diagnosis & Treatment of Circulatory Shock 🚑💡
🔹 The key to precision resuscitation:
•Is the patient in compensated shock?
•Will cardiac output improve with fluids?
•What is the arterial tone status?
•Can the heart sustain output without filling pressures?
🔹 The key to precision resuscitation:
•Is the patient in compensated shock?
•Will cardiac output improve with fluids?
•What is the arterial tone status?
•Can the heart sustain output without filling pressures?

March 20, 2025 at 5:55 PM
#ISICEM25 | Michael R. Pinsky on Autonomous Diagnosis & Treatment of Circulatory Shock 🚑💡
🔹 The key to precision resuscitation:
•Is the patient in compensated shock?
•Will cardiac output improve with fluids?
•What is the arterial tone status?
•Can the heart sustain output without filling pressures?
🔹 The key to precision resuscitation:
•Is the patient in compensated shock?
•Will cardiac output improve with fluids?
•What is the arterial tone status?
•Can the heart sustain output without filling pressures?
#ISICEM25 | Michael Pinsky presents an algorithm for precise personalized resuscitation in shock management 🔄📊
🔹 Stepwise decision-making:
✅ Is the patient hemodynamically stable? If yes, do nothing.
✅ If unstable, assess preload responsiveness.
✅ If preload-responsive, evaluate vasomotor tone
🔹 Stepwise decision-making:
✅ Is the patient hemodynamically stable? If yes, do nothing.
✅ If unstable, assess preload responsiveness.
✅ If preload-responsive, evaluate vasomotor tone

March 20, 2025 at 5:55 PM
#ISICEM25 | Michael Pinsky presents an algorithm for precise personalized resuscitation in shock management 🔄📊
🔹 Stepwise decision-making:
✅ Is the patient hemodynamically stable? If yes, do nothing.
✅ If unstable, assess preload responsiveness.
✅ If preload-responsive, evaluate vasomotor tone
🔹 Stepwise decision-making:
✅ Is the patient hemodynamically stable? If yes, do nothing.
✅ If unstable, assess preload responsiveness.
✅ If preload-responsive, evaluate vasomotor tone
#ISICEM25 | Michael Pinsky on Functional Hemodynamic Monitoring & Closed-Loop Resuscitation 🔄📊
✅ Guided resuscitation with clear decision rules
✅ Standardized yet personalized fluid & vasopressor strategies
✅ Adaptable across ICUs, remote care, and austere environments
Looking at the future!
✅ Guided resuscitation with clear decision rules
✅ Standardized yet personalized fluid & vasopressor strategies
✅ Adaptable across ICUs, remote care, and austere environments
Looking at the future!

March 20, 2025 at 5:55 PM
#ISICEM25 | Michael Pinsky on Functional Hemodynamic Monitoring & Closed-Loop Resuscitation 🔄📊
✅ Guided resuscitation with clear decision rules
✅ Standardized yet personalized fluid & vasopressor strategies
✅ Adaptable across ICUs, remote care, and austere environments
Looking at the future!
✅ Guided resuscitation with clear decision rules
✅ Standardized yet personalized fluid & vasopressor strategies
✅ Adaptable across ICUs, remote care, and austere environments
Looking at the future!
#ISICEM25 | Lennie Derde on the future of sepsis treatment 🔬🦠
🚀 Moving beyond syndromes to treatable traits
🔹 Reframing immunobiology for better-targeted therapies
🎯 Immune modulation: precision over generalization
🧬 Metabolic reprogramming—a new frontier?
🚀 Moving beyond syndromes to treatable traits
🔹 Reframing immunobiology for better-targeted therapies
🎯 Immune modulation: precision over generalization
🧬 Metabolic reprogramming—a new frontier?


March 20, 2025 at 5:55 PM
#ISICEM25 | Lennie Derde on the future of sepsis treatment 🔬🦠
🚀 Moving beyond syndromes to treatable traits
🔹 Reframing immunobiology for better-targeted therapies
🎯 Immune modulation: precision over generalization
🧬 Metabolic reprogramming—a new frontier?
🚀 Moving beyond syndromes to treatable traits
🔹 Reframing immunobiology for better-targeted therapies
🎯 Immune modulation: precision over generalization
🧬 Metabolic reprogramming—a new frontier?


#ISICEM25 | @fabio_taccone delivers a brilliantly clear presentation on Automated Pupillometry 👁️💡
"The conclusion is quite simple: If you think measuring pupils makes sense, the pupillometer is better than you!"
🔹 Objective, reproducible, and precise
🔹 Eliminates subjectivity in pupil assessment
"The conclusion is quite simple: If you think measuring pupils makes sense, the pupillometer is better than you!"
🔹 Objective, reproducible, and precise
🔹 Eliminates subjectivity in pupil assessment


March 20, 2025 at 5:55 PM
#ISICEM25 | @fabio_taccone delivers a brilliantly clear presentation on Automated Pupillometry 👁️💡
"The conclusion is quite simple: If you think measuring pupils makes sense, the pupillometer is better than you!"
🔹 Objective, reproducible, and precise
🔹 Eliminates subjectivity in pupil assessment
"The conclusion is quite simple: If you think measuring pupils makes sense, the pupillometer is better than you!"
🔹 Objective, reproducible, and precise
🔹 Eliminates subjectivity in pupil assessment
#ISICEM25 | Massimiliano Greco on wearable technologies and the future of ICU monitoring! 🚀📡
🔹 Increase mobility & physical therapy
🔹 Reduce invasive devices & sampling
🔹 Improve data visualization & reduce fatigue
🔹 Detect delirium earlier
🔹 Bridge monitoring gaps between ICU & wards
🔹 Increase mobility & physical therapy
🔹 Reduce invasive devices & sampling
🔹 Improve data visualization & reduce fatigue
🔹 Detect delirium earlier
🔹 Bridge monitoring gaps between ICU & wards


March 20, 2025 at 1:16 PM
#ISICEM25 | Massimiliano Greco on wearable technologies and the future of ICU monitoring! 🚀📡
🔹 Increase mobility & physical therapy
🔹 Reduce invasive devices & sampling
🔹 Improve data visualization & reduce fatigue
🔹 Detect delirium earlier
🔹 Bridge monitoring gaps between ICU & wards
🔹 Increase mobility & physical therapy
🔹 Reduce invasive devices & sampling
🔹 Improve data visualization & reduce fatigue
🔹 Detect delirium earlier
🔹 Bridge monitoring gaps between ICU & wards
#ISICEM25 | 🚀 The session ‘HOW I IMAGINE THE FUTURE’ is now starting! Moderated by Zsolt Molnar & Christian Stoppe, this session explores bold visions for the future of intensive care.

March 20, 2025 at 1:02 PM
#ISICEM25 | 🚀 The session ‘HOW I IMAGINE THE FUTURE’ is now starting! Moderated by Zsolt Molnar & Christian Stoppe, this session explores bold visions for the future of intensive care.
#ISICEM25 | 🔥 Big debate in the room!
After the first fluid challenge in septic shock, BP rises from 90/40 to 95/45. What’s the next move?
More fluids 💧 or start vasopressors 💉
After the first fluid challenge in septic shock, BP rises from 90/40 to 95/45. What’s the next move?
More fluids 💧 or start vasopressors 💉

March 20, 2025 at 10:19 AM
#ISICEM25 | 🔥 Big debate in the room!
After the first fluid challenge in septic shock, BP rises from 90/40 to 95/45. What’s the next move?
More fluids 💧 or start vasopressors 💉
After the first fluid challenge in septic shock, BP rises from 90/40 to 95/45. What’s the next move?
More fluids 💧 or start vasopressors 💉
#ISICEM25 | 🔴 Live from the Arch Room! The Round Table on Early Hemodynamic Resuscitation of Septic Shock is underway.
🗣️ Moderator: Xavier Monnet
💡 Experts: Daniel De Backer, Emily J See, Jean-Louis Teboul, Michelle Chew
🗣️ Moderator: Xavier Monnet
💡 Experts: Daniel De Backer, Emily J See, Jean-Louis Teboul, Michelle Chew

March 20, 2025 at 10:19 AM
#ISICEM25 | 🔴 Live from the Arch Room! The Round Table on Early Hemodynamic Resuscitation of Septic Shock is underway.
🗣️ Moderator: Xavier Monnet
💡 Experts: Daniel De Backer, Emily J See, Jean-Louis Teboul, Michelle Chew
🗣️ Moderator: Xavier Monnet
💡 Experts: Daniel De Backer, Emily J See, Jean-Louis Teboul, Michelle Chew