
AndrewFolpe
@folpe-mn-st.bsky.social
350 followers
74 following
230 posts
I like my wife and family, bikes, music, dogs, baking bread and soft tissue tumors. Only the last here though.
Posts
Media
Videos
Starter Packs

AndrewFolpe
@folpe-mn-st.bsky.social
· Jun 12
GLI1 Coamplification in Well-Differentiated/Dedifferentiated Liposarcomas: Clinicopathologic and Molecular Analysis of 92 Cases - PubMed
GLI1(12q13.3) amplification is identified in a subset of mesenchymal neoplasms with a distinct nested round cell/epithelioid phenotype. MDM2 and CDK4 genes are situated along the oncogenic 12q13-15 se...
pubmed.ncbi.nlm.nih.gov
AndrewFolpe
@folpe-mn-st.bsky.social
· Jun 12





AndrewFolpe
@folpe-mn-st.bsky.social
· Jun 12


AndrewFolpe
@folpe-mn-st.bsky.social
· Jun 5







AndrewFolpe
@folpe-mn-st.bsky.social
· May 30
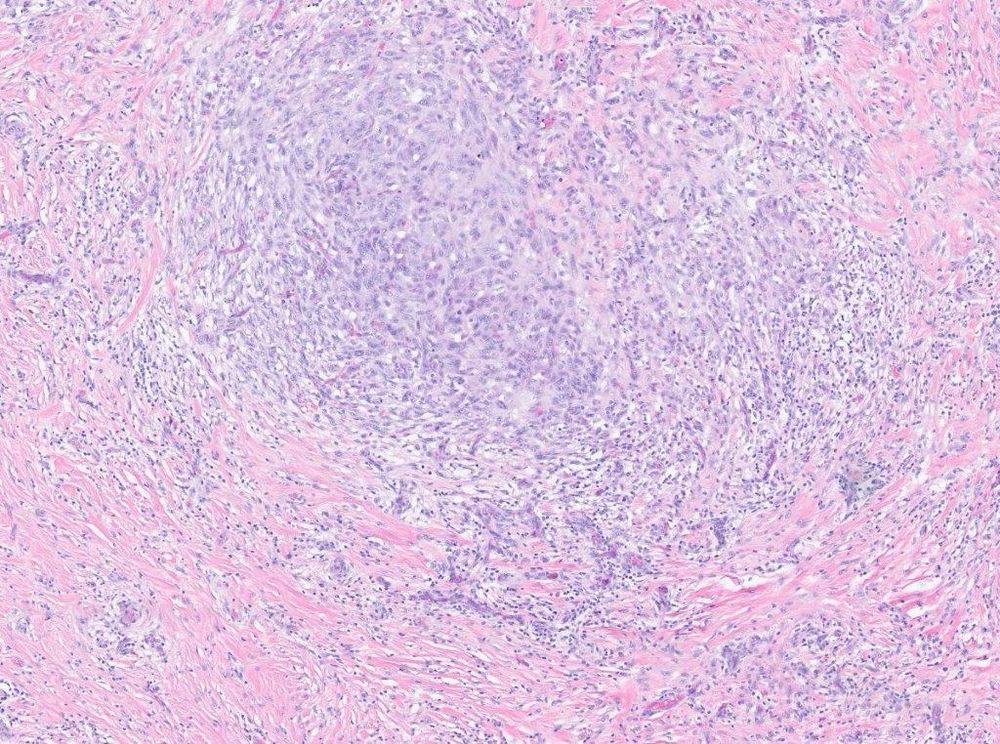
Desmoid Fibromatosis With TP53 Mutation and Striking Nuclear Pleomorphism - PubMed
Desmoid fibromatosis is a myofibroblastic neoplasm of intermediate biologic potential, which has a strong predilection for local recurrence but does not metastasize. Arranged in long, sweeping fascicl...
pubmed.ncbi.nlm.nih.gov










AndrewFolpe
@folpe-mn-st.bsky.social
· May 23
AndrewFolpe
@folpe-mn-st.bsky.social
· May 20


AndrewFolpe
@folpe-mn-st.bsky.social
· May 20
A Novel SS18-SSX Fusion-specific Antibody for the Diagnosis of Synovial Sarcoma - PubMed
Synovial sarcoma (SS), an aggressive soft tissue sarcoma with a predilection for the extremities of young adults, harbors the pathognomonic t(X;18)(p11;q11) translocation, resulting in SS18-SSX rearra...
pubmed.ncbi.nlm.nih.gov



AndrewFolpe
@folpe-mn-st.bsky.social
· May 15
AndrewFolpe
@folpe-mn-st.bsky.social
· May 15

AndrewFolpe
@folpe-mn-st.bsky.social
· May 14
Dedifferentiated Liposarcoma With Epithelioid/Epithelial Features - PubMed
Dedifferentiated liposarcoma (DDLPS) demonstrates a variety of growth patterns, and their histologic resemblance to other spindle cell mesenchymal tumors has been widely recognized. However, epithelio...
pubmed.ncbi.nlm.nih.gov
AndrewFolpe
@folpe-mn-st.bsky.social
· May 14
AndrewFolpe
@folpe-mn-st.bsky.social
· May 14