




Isaac Lamb, MD
@isaaclamb01.bsky.social
PGY-4 neurology resident. Interested in clinical neurology, medical education, history, and nerd stuff.
Image references:
1. DOI: 10.1586/17474086.2014.954541
2. DOI: 10.1016/j.amjmed.2020.03.005
3. my.clevelandclinic.org/health/disea...
4. my.clevelandclinic.org/health/diagn...
5. www.irhythmtech.com/us/en
1. DOI: 10.1586/17474086.2014.954541
2. DOI: 10.1016/j.amjmed.2020.03.005
3. my.clevelandclinic.org/health/disea...
4. my.clevelandclinic.org/health/diagn...
5. www.irhythmtech.com/us/en
Patent Foramen Ovale: What It Is and How Serious It Can Be
Patent foramen ovale is a normal feature in your newborn’s heart. But when they still have it past age 3, it might need treatment. Learn more about this condition and its treatment.
my.clevelandclinic.org
July 12, 2025 at 8:52 PM
Image references:
1. DOI: 10.1586/17474086.2014.954541
2. DOI: 10.1016/j.amjmed.2020.03.005
3. my.clevelandclinic.org/health/disea...
4. my.clevelandclinic.org/health/diagn...
5. www.irhythmtech.com/us/en
1. DOI: 10.1586/17474086.2014.954541
2. DOI: 10.1016/j.amjmed.2020.03.005
3. my.clevelandclinic.org/health/disea...
4. my.clevelandclinic.org/health/diagn...
5. www.irhythmtech.com/us/en
SUMMARY:
- Imaging: strokes in multiple territories
- Workup: TTE with bubble, cardiac monitoring, +/- TEE
- Management
> Afib: AC (DOAC preferred) vs LAA occlusion
> PFO: refer for closure if high risk
> Ventricular thrombus: warfarin
- Imaging: strokes in multiple territories
- Workup: TTE with bubble, cardiac monitoring, +/- TEE
- Management
> Afib: AC (DOAC preferred) vs LAA occlusion
> PFO: refer for closure if high risk
> Ventricular thrombus: warfarin
July 12, 2025 at 8:52 PM
SUMMARY:
- Imaging: strokes in multiple territories
- Workup: TTE with bubble, cardiac monitoring, +/- TEE
- Management
> Afib: AC (DOAC preferred) vs LAA occlusion
> PFO: refer for closure if high risk
> Ventricular thrombus: warfarin
- Imaging: strokes in multiple territories
- Workup: TTE with bubble, cardiac monitoring, +/- TEE
- Management
> Afib: AC (DOAC preferred) vs LAA occlusion
> PFO: refer for closure if high risk
> Ventricular thrombus: warfarin
I’ll point out that there are other central embolic strokes that we didn’t talk about here because I’m planning to discuss them later:
- ESUS (cryptogenic)
- Septic embolism / endocarditis
- Arterial hypercoagulability
Stay tuned for a future thread on these!
- ESUS (cryptogenic)
- Septic embolism / endocarditis
- Arterial hypercoagulability
Stay tuned for a future thread on these!
July 12, 2025 at 8:52 PM
I’ll point out that there are other central embolic strokes that we didn’t talk about here because I’m planning to discuss them later:
- ESUS (cryptogenic)
- Septic embolism / endocarditis
- Arterial hypercoagulability
Stay tuned for a future thread on these!
- ESUS (cryptogenic)
- Septic embolism / endocarditis
- Arterial hypercoagulability
Stay tuned for a future thread on these!
Ventricular thrombi and valvular afib have not been as well studied. Current AHA guidelines recommend warfarin over DOACs but this is mostly due to a paucity of evidence.
July 12, 2025 at 8:52 PM
Ventricular thrombi and valvular afib have not been as well studied. Current AHA guidelines recommend warfarin over DOACs but this is mostly due to a paucity of evidence.
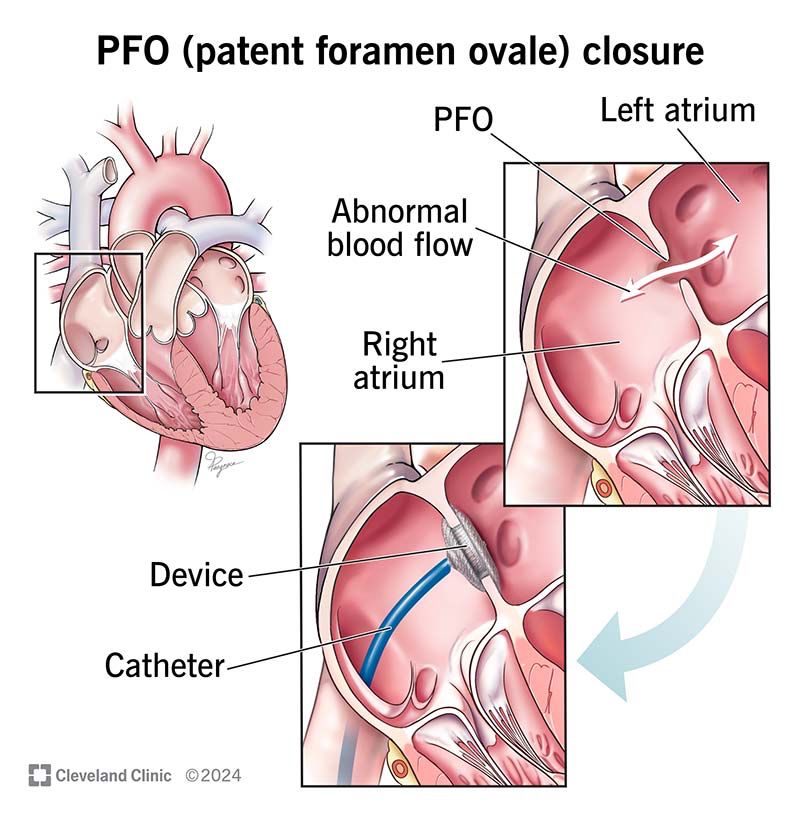
Should you close a PFO?
Not necessarily. About 20% of the population has a PFO. Most strokes, even in patients with a PFO, were probably from something else.
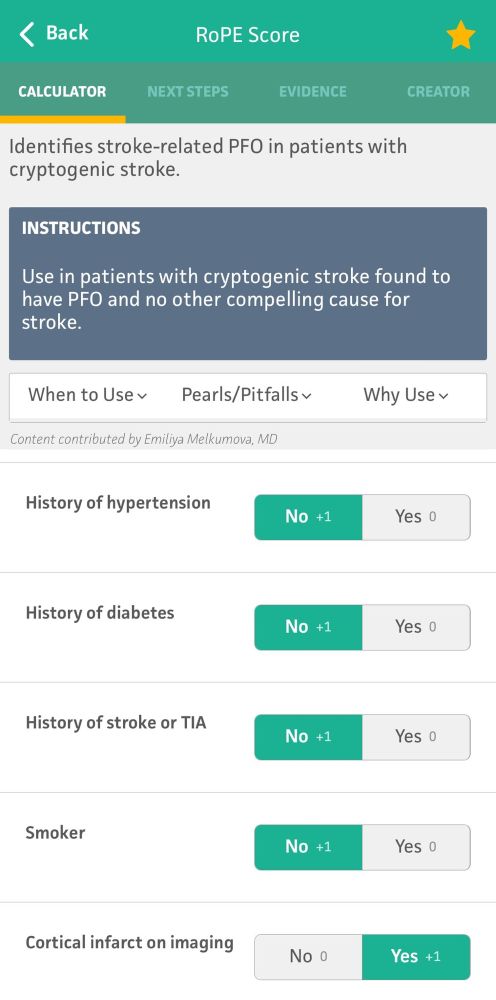
The decision to close one is based off of size, imaging, patient age and risk, and scoring tools (eg RoPE score).
Not necessarily. About 20% of the population has a PFO. Most strokes, even in patients with a PFO, were probably from something else.
The decision to close one is based off of size, imaging, patient age and risk, and scoring tools (eg RoPE score).
July 12, 2025 at 8:52 PM
Should you close a PFO?
Not necessarily. About 20% of the population has a PFO. Most strokes, even in patients with a PFO, were probably from something else.
The decision to close one is based off of size, imaging, patient age and risk, and scoring tools (eg RoPE score).
Not necessarily. About 20% of the population has a PFO. Most strokes, even in patients with a PFO, were probably from something else.
The decision to close one is based off of size, imaging, patient age and risk, and scoring tools (eg RoPE score).
The decision to cardiovert is another important one. Options include both chemical and electrical cardioversion and generally requires either short term anticoagulation or a TEE to exclude thrombus. Generally, this decision is up to the cardiologist.
July 12, 2025 at 8:52 PM
The decision to cardiovert is another important one. Options include both chemical and electrical cardioversion and generally requires either short term anticoagulation or a TEE to exclude thrombus. Generally, this decision is up to the cardiologist.
TREATMENT
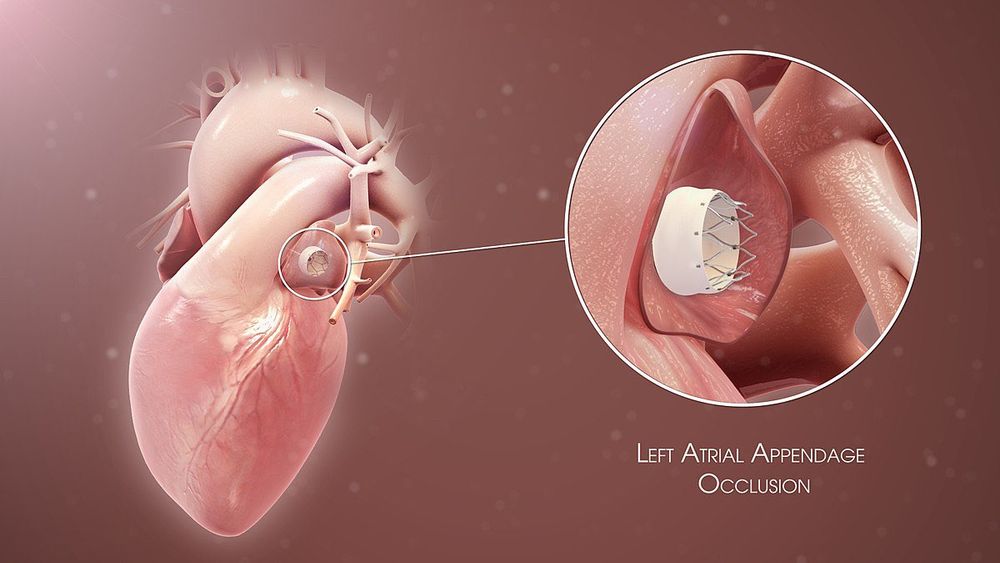
Most afib patients require chronic anticoagulation, and this is doubly true for stroke patients. Studies have shown superiority in DOACs (eg apixaban) over warfarin. If patients have contraindications to chronic AC, a LAA occlusive device gets almost the same benefit.
Most afib patients require chronic anticoagulation, and this is doubly true for stroke patients. Studies have shown superiority in DOACs (eg apixaban) over warfarin. If patients have contraindications to chronic AC, a LAA occlusive device gets almost the same benefit.
July 12, 2025 at 8:52 PM
TREATMENT
Most afib patients require chronic anticoagulation, and this is doubly true for stroke patients. Studies have shown superiority in DOACs (eg apixaban) over warfarin. If patients have contraindications to chronic AC, a LAA occlusive device gets almost the same benefit.
Most afib patients require chronic anticoagulation, and this is doubly true for stroke patients. Studies have shown superiority in DOACs (eg apixaban) over warfarin. If patients have contraindications to chronic AC, a LAA occlusive device gets almost the same benefit.
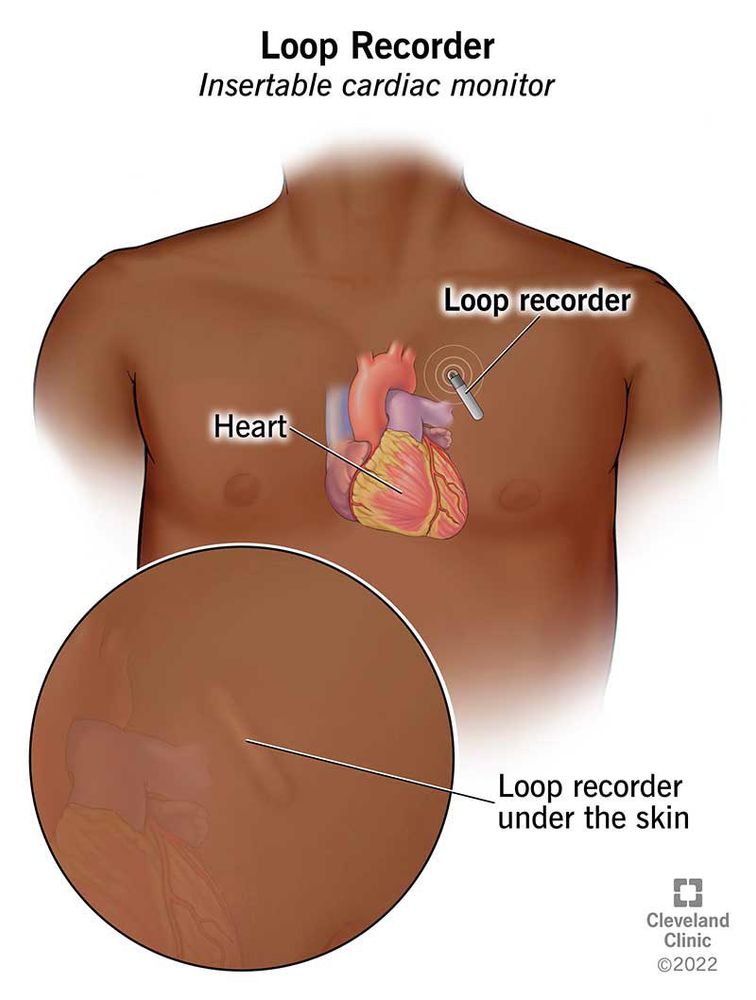
While we monitor all stroke patients while inpatient, statistically many cases of afib are paroxysmal and will be missed. We use a variety of ambulatory cardiac monitoring devices on discharge to improve sensitivity.

July 12, 2025 at 8:52 PM
While we monitor all stroke patients while inpatient, statistically many cases of afib are paroxysmal and will be missed. We use a variety of ambulatory cardiac monitoring devices on discharge to improve sensitivity.
Afib can be detected as easily as via a simple EKG, but interpretation is tricky. What if they were only in afib for a few minutes secondary to heart strain from the stroke? Or what if they are back in NSR?
July 12, 2025 at 8:52 PM
Afib can be detected as easily as via a simple EKG, but interpretation is tricky. What if they were only in afib for a few minutes secondary to heart strain from the stroke? Or what if they are back in NSR?
Emerging diagnostic modalities include cardiac CT, which has shown particular value for identifying ventricular thrombus and doesn’t come with the procedural risks of TEE.
July 12, 2025 at 8:52 PM
Emerging diagnostic modalities include cardiac CT, which has shown particular value for identifying ventricular thrombus and doesn’t come with the procedural risks of TEE.
If we have a high suspicion for either LAA thrombus or PFO, obtaining a TEE may be needed. It gets a closer look at the left atrium but comes procedural risks.
July 12, 2025 at 8:52 PM
If we have a high suspicion for either LAA thrombus or PFO, obtaining a TEE may be needed. It gets a closer look at the left atrium but comes procedural risks.
While getting a TTE, we almost always inject agitated saline contrast to look for a PFO. If no PFO is seen, we can usually exclude paradoxical embolus. If we see one, we may have to go DVT hunting in the limbs and pelvis via ultrasound and/or MRV/CTV.
July 12, 2025 at 8:52 PM
While getting a TTE, we almost always inject agitated saline contrast to look for a PFO. If no PFO is seen, we can usually exclude paradoxical embolus. If we see one, we may have to go DVT hunting in the limbs and pelvis via ultrasound and/or MRV/CTV.
TTEs are good at excluding ventricular thrombi but don’t get a good look at the left atrial appendage (LAA), which is where 90% of clots form in afib.
It can also show chronic atrial disease, low ejection fraction, valvular issues, and other thrombogenic conditions.
It can also show chronic atrial disease, low ejection fraction, valvular issues, and other thrombogenic conditions.
July 12, 2025 at 8:52 PM
TTEs are good at excluding ventricular thrombi but don’t get a good look at the left atrial appendage (LAA), which is where 90% of clots form in afib.
It can also show chronic atrial disease, low ejection fraction, valvular issues, and other thrombogenic conditions.
It can also show chronic atrial disease, low ejection fraction, valvular issues, and other thrombogenic conditions.
DIAGNOSIS
To detect these strokes, we use two types of tools: electrical (EKG with/without ambulatory monitoring) and structural (TTE +/- TEE).
To detect these strokes, we use two types of tools: electrical (EKG with/without ambulatory monitoring) and structural (TTE +/- TEE).
July 12, 2025 at 8:52 PM
DIAGNOSIS
To detect these strokes, we use two types of tools: electrical (EKG with/without ambulatory monitoring) and structural (TTE +/- TEE).
To detect these strokes, we use two types of tools: electrical (EKG with/without ambulatory monitoring) and structural (TTE +/- TEE).
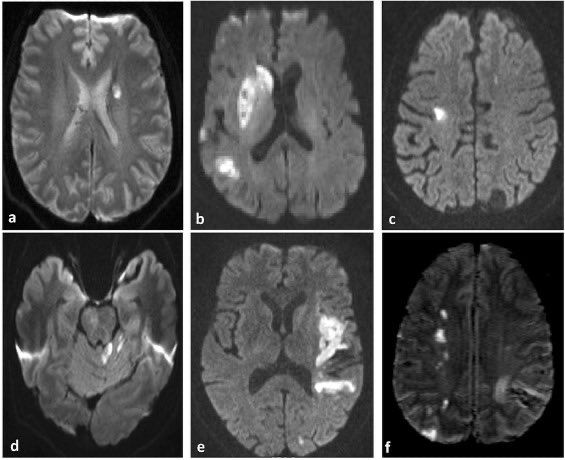
Sometimes you will see strokes of different ages on MRI, suggesting the heart is flinging out multiple clots over a period of time. When these fall in variable vascular territories, it strongly suggests a central (cardio) embolic source.
July 12, 2025 at 8:52 PM
Sometimes you will see strokes of different ages on MRI, suggesting the heart is flinging out multiple clots over a period of time. When these fall in variable vascular territories, it strongly suggests a central (cardio) embolic source.
IMAGING
The thrombi from cardioembolic strokes are typically larger than atheroembolic strokes (see pt 1) meaning the strokes generally fall in large vessel territories (not lacunes).
The unique feature is that it can hit any vascular territory, left/right/anterior posterior.
The thrombi from cardioembolic strokes are typically larger than atheroembolic strokes (see pt 1) meaning the strokes generally fall in large vessel territories (not lacunes).
The unique feature is that it can hit any vascular territory, left/right/anterior posterior.
July 12, 2025 at 8:52 PM
IMAGING
The thrombi from cardioembolic strokes are typically larger than atheroembolic strokes (see pt 1) meaning the strokes generally fall in large vessel territories (not lacunes).
The unique feature is that it can hit any vascular territory, left/right/anterior posterior.
The thrombi from cardioembolic strokes are typically larger than atheroembolic strokes (see pt 1) meaning the strokes generally fall in large vessel territories (not lacunes).
The unique feature is that it can hit any vascular territory, left/right/anterior posterior.
Some of the more important causes include:
- afib/aflutter
- paradoxical embolism via patent foramen ovale (PFO)
- ventricular thrombus
- valvular stenosis
- afib/aflutter
- paradoxical embolism via patent foramen ovale (PFO)
- ventricular thrombus
- valvular stenosis
July 12, 2025 at 8:52 PM
Some of the more important causes include:
- afib/aflutter
- paradoxical embolism via patent foramen ovale (PFO)
- ventricular thrombus
- valvular stenosis
- afib/aflutter
- paradoxical embolism via patent foramen ovale (PFO)
- ventricular thrombus
- valvular stenosis
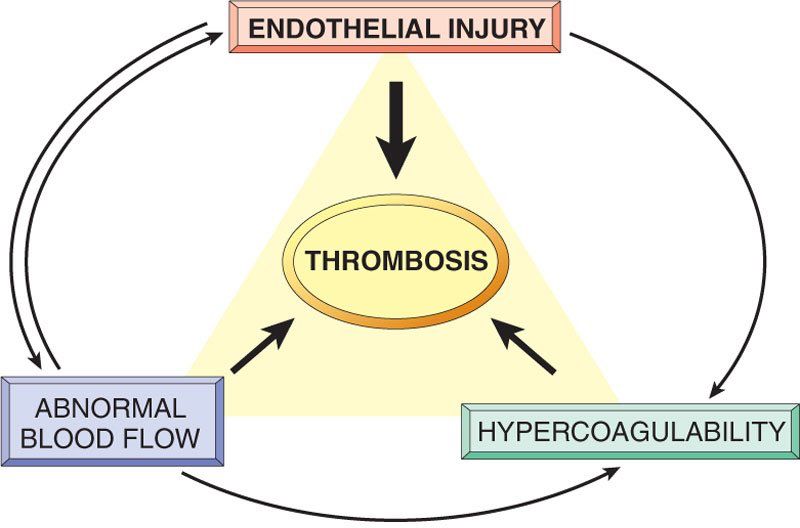
PATHOPHYSIOLOGY
Cardioembolic strokes are generally caused by the other two corners of Virchow’s triad: stasis (eg afib) and hypercoagulability (eg paradoxical embolus from a DVT). Overactivity of secondary coagulation results in a thrombus which can embolize.
Cardioembolic strokes are generally caused by the other two corners of Virchow’s triad: stasis (eg afib) and hypercoagulability (eg paradoxical embolus from a DVT). Overactivity of secondary coagulation results in a thrombus which can embolize.
July 12, 2025 at 8:52 PM
PATHOPHYSIOLOGY
Cardioembolic strokes are generally caused by the other two corners of Virchow’s triad: stasis (eg afib) and hypercoagulability (eg paradoxical embolus from a DVT). Overactivity of secondary coagulation results in a thrombus which can embolize.
Cardioembolic strokes are generally caused by the other two corners of Virchow’s triad: stasis (eg afib) and hypercoagulability (eg paradoxical embolus from a DVT). Overactivity of secondary coagulation results in a thrombus which can embolize.
My panoptic was money well spent though! I’m trash without it, but I feel pretty good about fundoscopy skills now. I bought it for cheap as an MS4 off of another med student who unwisely bought one before going into anesthesia.
July 7, 2025 at 10:11 PM
My panoptic was money well spent though! I’m trash without it, but I feel pretty good about fundoscopy skills now. I bought it for cheap as an MS4 off of another med student who unwisely bought one before going into anesthesia.
I use mine for pupil assessment. I learned early on that you will never catch subtle anisocoria or an rAPD with a phone light. Need something bright and focused.
July 7, 2025 at 10:09 PM
I use mine for pupil assessment. I learned early on that you will never catch subtle anisocoria or an rAPD with a phone light. Need something bright and focused.
Image sources:
1. DOI: 10.1161/01.str.24.1.35
2. DOI: 10.1136/svn-2016-000035
3. DOI: 10.1016/j.jstrokecerebrovasdis.2018.02.010
4. DOI: 10.1001/jamaneurol.2018.1073
5. DOI: 10.1111/nan.12472
6. DOI: 10.1016/j.nicl.2023.103480
7. DOI: 10.1586/17474086.2014.954541
1. DOI: 10.1161/01.str.24.1.35
2. DOI: 10.1136/svn-2016-000035
3. DOI: 10.1016/j.jstrokecerebrovasdis.2018.02.010
4. DOI: 10.1001/jamaneurol.2018.1073
5. DOI: 10.1111/nan.12472
6. DOI: 10.1016/j.nicl.2023.103480
7. DOI: 10.1586/17474086.2014.954541
July 7, 2025 at 10:06 PM
Image sources:
1. DOI: 10.1161/01.str.24.1.35
2. DOI: 10.1136/svn-2016-000035
3. DOI: 10.1016/j.jstrokecerebrovasdis.2018.02.010
4. DOI: 10.1001/jamaneurol.2018.1073
5. DOI: 10.1111/nan.12472
6. DOI: 10.1016/j.nicl.2023.103480
7. DOI: 10.1586/17474086.2014.954541
1. DOI: 10.1161/01.str.24.1.35
2. DOI: 10.1136/svn-2016-000035
3. DOI: 10.1016/j.jstrokecerebrovasdis.2018.02.010
4. DOI: 10.1001/jamaneurol.2018.1073
5. DOI: 10.1111/nan.12472
6. DOI: 10.1016/j.nicl.2023.103480
7. DOI: 10.1586/17474086.2014.954541
RECAP:
- Acute: lacunar syndromes
- Chronic: vascular dementia
- Imaging: lacunes in the deep white and gray, white matter hyperintensities
- Path: arteriosclerosis and branch atheroma
- Risk factors: HTN, diabetes
- Treatment: antiplatelets, risk factor control
- Acute: lacunar syndromes
- Chronic: vascular dementia
- Imaging: lacunes in the deep white and gray, white matter hyperintensities
- Path: arteriosclerosis and branch atheroma
- Risk factors: HTN, diabetes
- Treatment: antiplatelets, risk factor control
July 7, 2025 at 10:06 PM
RECAP:
- Acute: lacunar syndromes
- Chronic: vascular dementia
- Imaging: lacunes in the deep white and gray, white matter hyperintensities
- Path: arteriosclerosis and branch atheroma
- Risk factors: HTN, diabetes
- Treatment: antiplatelets, risk factor control
- Acute: lacunar syndromes
- Chronic: vascular dementia
- Imaging: lacunes in the deep white and gray, white matter hyperintensities
- Path: arteriosclerosis and branch atheroma
- Risk factors: HTN, diabetes
- Treatment: antiplatelets, risk factor control
Traditional vascular risk factor mitigation is crucial, most importantly diabetes and hypertension.
These patients are also treated with lifelong single antiplatelet therapy (remember Virchow’s triad).
DAPT has a slight benefit but only in the very short term (ie 21 days).
These patients are also treated with lifelong single antiplatelet therapy (remember Virchow’s triad).
DAPT has a slight benefit but only in the very short term (ie 21 days).
July 7, 2025 at 10:06 PM
Traditional vascular risk factor mitigation is crucial, most importantly diabetes and hypertension.
These patients are also treated with lifelong single antiplatelet therapy (remember Virchow’s triad).
DAPT has a slight benefit but only in the very short term (ie 21 days).
These patients are also treated with lifelong single antiplatelet therapy (remember Virchow’s triad).
DAPT has a slight benefit but only in the very short term (ie 21 days).
TREATMENT
Like most ischemic strokes, lacunar syndromes can improve with thrombolytic therapy (ie tPA) in the right time window. By definition, the vessels are too small for thrombectomy, though.
Like most ischemic strokes, lacunar syndromes can improve with thrombolytic therapy (ie tPA) in the right time window. By definition, the vessels are too small for thrombectomy, though.
July 7, 2025 at 10:06 PM
TREATMENT
Like most ischemic strokes, lacunar syndromes can improve with thrombolytic therapy (ie tPA) in the right time window. By definition, the vessels are too small for thrombectomy, though.
Like most ischemic strokes, lacunar syndromes can improve with thrombolytic therapy (ie tPA) in the right time window. By definition, the vessels are too small for thrombectomy, though.