



AI enables real-time, personalized healthcare decisions
Edition-2: Artificial Intelligence (AI) in Medicine – AIIM 2026
May 04–05, 2026
Boston, Massachusetts, USA
🌐 ai-medicalcongress.com
#AIIM2026 #AIinMedicine #MedicalAI #DigitalHealth #ClinicalDecisionSupport #WearableAI #HealthcareInnovation
Edition-2: Artificial Intelligence (AI) in Medicine – AIIM 2026
May 04–05, 2026
Boston, Massachusetts, USA
🌐 ai-medicalcongress.com
#AIIM2026 #AIinMedicine #MedicalAI #DigitalHealth #ClinicalDecisionSupport #WearableAI #HealthcareInnovation

December 15, 2025 at 12:45 PM
AI enables real-time, personalized healthcare decisions
Edition-2: Artificial Intelligence (AI) in Medicine – AIIM 2026
May 04–05, 2026
Boston, Massachusetts, USA
🌐 ai-medicalcongress.com
#AIIM2026 #AIinMedicine #MedicalAI #DigitalHealth #ClinicalDecisionSupport #WearableAI #HealthcareInnovation
Edition-2: Artificial Intelligence (AI) in Medicine – AIIM 2026
May 04–05, 2026
Boston, Massachusetts, USA
🌐 ai-medicalcongress.com
#AIIM2026 #AIinMedicine #MedicalAI #DigitalHealth #ClinicalDecisionSupport #WearableAI #HealthcareInnovation

JMIR Formative Res: Evaluating a Clinical Decision Support Tool for #Cancer Risk Assessment in Primary Care: Simulation Study of Unintended Weight Loss #Cancer #HealthTech #ClinicalDecisionSupport #PrimaryCare #WeightLoss

Evaluating a Clinical Decision Support Tool for #Cancer Risk Assessment in Primary Care: Simulation Study of Unintended Weight Loss
Background: Early #Cancer detection is crucial, but recognising the significance of associated symptoms such as unintended weight loss in primary care remains challenging. Clinical Decision Support Systems (CDSS) can aid #Cancer detection, but face implementation barriers and low uptake in real-world settings. To address these issues, simulation environments offer a controlled setting to study CDSS usage and improve their design for better adoption in clinical practice. Objective: To evaluate a CDSS integrated within general practice electronic health records aimed at identifying patients at risk of undiagnosed #Cancer. Methods: The evaluation of CDSS to identify patients with unintended weight loss was conducted in a simulated primary care environment where GPs interacted with the CDSS in simulated clinical consultations. There were four possible clinical scenarios based on patient gender and risk of #Cancer. Data collection included interviews with GPs, #Cancer survivors (lived-experience community advocates), and patient actors, as well as video analysis of GP-CDSS interactions. Two theoretical frameworks were employed for thematic interpretation of the data. Results: We recruited 10 GPs and 6 community advocates, conducting 20 simulated consultations with two patient actors (two consultations per GP, one high-risk and one low-risk). All participants found the CDSS acceptable and unobtrusive. GPs utilised CDSS recommendations in three distinct ways: as a communication aid when discussing follow up with the patient, as a reminder for differential diagnoses and recommended investigations, and as an aid to diagnostic decision-making without sharing with patients. The CDSS's impact on patient-doctor communication varied, both facilitating and hindering interactions depending on the GP's communication style. Conclusions: We developed and evaluated a CDSS for identifying #Cancer risk in patients with unintended weight loss in a simulated environment, revealing its potential to aid clinical decision-making and communication, while highlighting implementation challenges and the need for context-sensitive application. Clinical Trial: NA
dlvr.it
December 10, 2025 at 9:18 PM
JMIR Formative Res: Evaluating a Clinical Decision Support Tool for #Cancer Risk Assessment in Primary Care: Simulation Study of Unintended Weight Loss #Cancer #HealthTech #ClinicalDecisionSupport #PrimaryCare #WeightLoss
New in JMIR Nursing: An Expert Knowledge Algorithm and Model Predicting Wound Healing Trends for a Decision Support System for Pressure Injury Management in Home Care Nursing: Development and Validation Study #Nursing #Healthcare #WoundCare #PressureInjury #ClinicalDecisionSupport

An Expert Knowledge Algorithm and Model Predicting Wound Healing Trends for a Decision Support System for Pressure Injury Management in Home Care Nursing: Development and Validation Study
Background: Home-visiting #nurses have difficulty selecting appropriate pressure injury (PI) management despite using clinical practice guidelines in various home-visiting settings. Clinical decision support systems (CDSS) can help home-visiting #nurses’ decision-making. Objective: This study aimed to develop a care algorithm reflecting the expertise of a wound expert #nurse and a predictive model for the change of PI severity to inform home-visiting #nurses to receive actual consultation. Methods: First, an existing algorithm was modified by semi-structured interviews with a certified wound expert #nurse. Case information was input into both base and high-expertise algorithms, which provided care recommendations across nine fields: 1) pressure relief, 2) nutritional management, 3) shear relief, 4) moisture management, 5) wound dressing use, 6) care for physical factors including bone prominence, obesity, joint contractures, and periwound edema, 7) care for systemic disorder, 8) selection of wound dressings, ointments, and negative pressure wound therapy, and 9) wound cleansing. An expert interviewee assessed the high-expertise algorithm’s recommendations on a five-point scale, comparing them to the base algorithm and their own clinical judgment. To measure the algorithm’s applicability, agreement proportions were calculated as the number of vignettes where the care recommendation was considered appropriate/total number of vignettes. To measure the algorithm’s alignment, improvement proportions were calculated as the number of vignettes where the care recommendation improved/total number of vignettes excluding vignettes when the existing and high-expertise algorithm both showed an appropriate recommendation. Expected healing levels were evaluated by a 4-point scale where four indicates the high-expertise algorithm can “much improve” the case. Second, predictive distributions of changes of DESIGN-R®2020 score, PI severity score, were estimated with a hierarchical Bayesian model. The best model determined using training data (n=42) calculated coverage probabilities of 90% prediction interval in test data (n=34). The coverage probability of 90% prediction interval was defined as follows: the number of times when actual scores were within the 90% prediction interval/the number of assessments when the prediction was conducted. Results: The agreement proportions were 0.92, 0.75, and 0.89, respectively. The improvement proportions were 0.73, 0.25, and 0.76, respectively. The expected healing level was 2.67, 3.00, and 3.25, respectively. Coverage probabilities of 90% prediction interval in the test data were 0.67, 0.83, 0.86, and 0.80, respectively. Conclusions: This study developed an algorithm reflecting the expertise and a model to estimate predictive distributions of changes of DESIGN-R®2020 score for developing clinically applicable CDSS for home-visiting #nurses providing appropriate PI management. Clinical Trial: Not applicable.
dlvr.it
December 9, 2025 at 8:32 PM
New in JMIR Nursing: An Expert Knowledge Algorithm and Model Predicting Wound Healing Trends for a Decision Support System for Pressure Injury Management in Home Care Nursing: Development and Validation Study #Nursing #Healthcare #WoundCare #PressureInjury #ClinicalDecisionSupport

Guideline Adherence and Subjective Effects of a Mobile Clinical Decision Support System on Physicians' Practice: A Nationwide Survey-Based Within-Subject Study
E. C. d., J. G. V. d. et al.
Paper
Details
#ClinicalDecisionSupport #PhysicianPractice #HealthTechResearch
E. C. d., J. G. V. d. et al.
Paper
Details
#ClinicalDecisionSupport #PhysicianPractice #HealthTechResearch
December 6, 2025 at 9:02 AM
Guideline Adherence and Subjective Effects of a Mobile Clinical Decision Support System on Physicians' Practice: A Nationwide Survey-Based Within-Subject Study
E. C. d., J. G. V. d. et al.
Paper
Details
#ClinicalDecisionSupport #PhysicianPractice #HealthTechResearch
E. C. d., J. G. V. d. et al.
Paper
Details
#ClinicalDecisionSupport #PhysicianPractice #HealthTechResearch

NEW: A Two-Phase Framework Leveraging User Feedback and Systemic Validation to Improve Post-Live #ClinicalDecisionSupport
www.thieme-connect.de/products/ejo...
#MedSky #CDS #DigitalHealth
www.thieme-connect.de/products/ejo...
#MedSky #CDS #DigitalHealth

December 1, 2025 at 4:38 PM
NEW: A Two-Phase Framework Leveraging User Feedback and Systemic Validation to Improve Post-Live #ClinicalDecisionSupport
www.thieme-connect.de/products/ejo...
#MedSky #CDS #DigitalHealth
www.thieme-connect.de/products/ejo...
#MedSky #CDS #DigitalHealth
NEW: Effect of a #ClinicalDecisionSupport Tool for Identifying Patients Benefiting from #End-of-Life Discussions on #EmergencyDepartment Clinician Behavior www.thieme-connect.de/products/ejo...
#MedSky #CDS #PalliativeCare #DigitalHealth
#MedSky #CDS #PalliativeCare #DigitalHealth

December 1, 2025 at 4:34 PM
NEW: Effect of a #ClinicalDecisionSupport Tool for Identifying Patients Benefiting from #End-of-Life Discussions on #EmergencyDepartment Clinician Behavior www.thieme-connect.de/products/ejo...
#MedSky #CDS #PalliativeCare #DigitalHealth
#MedSky #CDS #PalliativeCare #DigitalHealth
November 13, 2025 at 4:01 PM
3➡️Une revue axée sur l’utilisation de l’IA dans les maladies infectieuses synthétisant ses applications actuelles et les défis à résoudre.
www.sciencedirect.com/science/arti...
#IDSky #IDSkyFr #InfectiousDiseases #AI #GenerativeArtificialIntelligence #MachineLearning #ClinicalDecisionSupport
www.sciencedirect.com/science/arti...
#IDSky #IDSkyFr #InfectiousDiseases #AI #GenerativeArtificialIntelligence #MachineLearning #ClinicalDecisionSupport
November 3, 2025 at 8:11 AM
3➡️Une revue axée sur l’utilisation de l’IA dans les maladies infectieuses synthétisant ses applications actuelles et les défis à résoudre.
www.sciencedirect.com/science/arti...
#IDSky #IDSkyFr #InfectiousDiseases #AI #GenerativeArtificialIntelligence #MachineLearning #ClinicalDecisionSupport
www.sciencedirect.com/science/arti...
#IDSky #IDSkyFr #InfectiousDiseases #AI #GenerativeArtificialIntelligence #MachineLearning #ClinicalDecisionSupport

RE.DOCTOR Vital Signs simplifies the capture, normalization, visualization, and routing of that data, helping clinicians detect deterioration earlier, reduce documentation burden, and make clearer, faster decisions.
Learn more and request a demo at re.doctor.
#VitalSigns #PatientMonitoring
Learn more and request a demo at re.doctor.
#VitalSigns #PatientMonitoring

October 19, 2025 at 2:41 AM
RE.DOCTOR Vital Signs simplifies the capture, normalization, visualization, and routing of that data, helping clinicians detect deterioration earlier, reduce documentation burden, and make clearer, faster decisions.
Learn more and request a demo at re.doctor.
#VitalSigns #PatientMonitoring
Learn more and request a demo at re.doctor.
#VitalSigns #PatientMonitoring
New in JMIR Aging: Evaluation of an AI-Based Clinical Decision Support System for Perioperative Care of Older Patients: Ethical Analysis of Focus Groups With Older Adults #AIHealthcare #ClinicalDecisionSupport #GeriatricCare #PerioperativeCare #EthicalAI

Evaluation of an AI-Based Clinical Decision Support System for Perioperative Care of Older Patients: Ethical Analysis of Focus Groups With Older Adults
Background: The development and introduction of an AI-based Clinical Decision Support System (CDSS) in surgical departments within the SURGE-Ahead project responds to the increasing aging population. Thereby, digital geriatric co-management with an evidence-based evaluation of the patient’s health condition and corresponding medical recommendations is aimed to improve the perioperative geriatric patient care. Objective: The use of an AI-based CDSS in patient care raises ethical challenges. The collection of opinions, expectations and concerns of older people as potential geriatric patients on the CDSS enables the identification of ethical chances, concerns and limitations that arise after implementing the technical device in hospitals. Methods: In total, five focus groups with participants aged 65 years and above were conducted. The transcripts were evaluated according to the qualitative content analysis and ethically analyzed: First, an inductive formation of categories was implemented, followed by a thematic classification of the participants’ statements. Thereby, we disproved technical understanding to impact the older people’s opinions. Results: Ethical chances and concerns were detected: The diagnosis and therapy could speed up, changes in the patient-AI-physician-interaction could improve medical treatment and enhance the coordination in hospitals. However, the quality of the CDSS depends on an adequate data basis and cyber security. A habituation effect and loss of a second medical option could develop, and the severity of an illness could be considered as an impact factor on the patient’s attitude towards medical suggestions. The risk of overdiagnosis and overtherapy was discussed controversially, and the range of therapy options could be influenced by interests and finances. Saving time resources would remain challenging, medical skills could decrease and the extent of the patient’s hospital stay could be affected. Conclusions: To respond to the ethical challenges, we recommend a time-sufficient use and emphasize an individual revision of the CDSS’s results. Furthermore, we suggest a limitation of private financial sponsoring.
dlvr.it
October 17, 2025 at 7:35 PM
New in JMIR Aging: Evaluation of an AI-Based Clinical Decision Support System for Perioperative Care of Older Patients: Ethical Analysis of Focus Groups With Older Adults #AIHealthcare #ClinicalDecisionSupport #GeriatricCare #PerioperativeCare #EthicalAI

The #ICE Advisory Group convened 30+ experts to address shifting #ClinicalGuidelines and their impact on #ClinicalDecisionSupport. @HLNConsulting shares key takeaways from this vital discussion: hln.com//ice-advisory-group-immunization-guidelines-2025.

ICE Advisory Group Reviews Evolving Immunization Guidelines | HLN
The Immunization Calculation Engine (ICE) Advisory Group met on September 29, 2025, bringing together over 30 experts to address evolving immunization guidelines, ACIP recommendations, and challenges ...
hln.com
October 6, 2025 at 8:17 PM
The #ICE Advisory Group convened 30+ experts to address shifting #ClinicalGuidelines and their impact on #ClinicalDecisionSupport. @HLNConsulting shares key takeaways from this vital discussion: hln.com//ice-advisory-group-immunization-guidelines-2025.

𝗜𝗻 𝗖𝗮𝘀𝗲 𝗬𝗼𝘂 𝗠𝗶𝘀𝘀𝗲𝗱 𝗜𝘁: #OncoscopeAI Founder & CEO Anna Forsythe new article in Forbes, "𝘍𝘳𝘰𝘮 𝘌𝘷𝘪𝘥𝘦𝘯𝘤𝘦 𝘛𝘰 #𝘈𝘐: 𝘞𝘩𝘺 𝘛𝘩𝘦 𝘍𝘶𝘵𝘶𝘳𝘦 𝘖𝘧 #𝘖𝘯𝘤𝘰𝘭𝘰𝘨𝘺 𝘋𝘦𝘤𝘪𝘴𝘪𝘰𝘯 𝘚𝘶𝘱𝘱𝘰𝘳𝘵 𝘔𝘶𝘴𝘵 𝘉𝘦 𝘉𝘶𝘪𝘭𝘵 𝘖𝘯 𝘓𝘪𝘷𝘪𝘯𝘨 𝘌𝘷𝘪𝘥𝘦𝘯𝘤𝘦"
Read the full article at the "News & Press" #LinkInBio.
#Cancer #ClinicalDecisionSupport #PrecisionMedicine
Read the full article at the "News & Press" #LinkInBio.
#Cancer #ClinicalDecisionSupport #PrecisionMedicine

September 26, 2025 at 4:42 PM
𝗜𝗻 𝗖𝗮𝘀𝗲 𝗬𝗼𝘂 𝗠𝗶𝘀𝘀𝗲𝗱 𝗜𝘁: #OncoscopeAI Founder & CEO Anna Forsythe new article in Forbes, "𝘍𝘳𝘰𝘮 𝘌𝘷𝘪𝘥𝘦𝘯𝘤𝘦 𝘛𝘰 #𝘈𝘐: 𝘞𝘩𝘺 𝘛𝘩𝘦 𝘍𝘶𝘵𝘶𝘳𝘦 𝘖𝘧 #𝘖𝘯𝘤𝘰𝘭𝘰𝘨𝘺 𝘋𝘦𝘤𝘪𝘴𝘪𝘰𝘯 𝘚𝘶𝘱𝘱𝘰𝘳𝘵 𝘔𝘶𝘴𝘵 𝘉𝘦 𝘉𝘶𝘪𝘭𝘵 𝘖𝘯 𝘓𝘪𝘷𝘪𝘯𝘨 𝘌𝘷𝘪𝘥𝘦𝘯𝘤𝘦"
Read the full article at the "News & Press" #LinkInBio.
#Cancer #ClinicalDecisionSupport #PrecisionMedicine
Read the full article at the "News & Press" #LinkInBio.
#Cancer #ClinicalDecisionSupport #PrecisionMedicine
JMIR Formative Res: Health Care Providers’ Perspectives of Clinical Decision Support Tools for Pediatric Sepsis in Bangladesh: Qualitative Study #Sepsis #PediatricHealthcare #DigitalHealth #mHealth #ClinicalDecisionSupport

Health Care Providers’ Perspectives of Clinical Decision Support Tools for Pediatric Sepsis in Bangladesh: Qualitative Study
Background: Sepsis, a life-threatening condition resulting from a dysregulated immune response to infection, disproportionately affects children in low- and middle-income countries (LMICs). Children with sepsis in LMICs face high mortality rates, with early detection and clinical monitoring posing significant challenges to effective management. There is great potential for digital technologies, such as wearable biosensor devices and mobile health (mHealth) clinical decision support (CDS) tools, together referred to as clinical decision support systems (CDSSs), to enable closer monitoring and more prompt recognition of children at risk of advanced sepsis and death. However, little is known about the perceptions of health care providers (HCPs) regarding the introduction of new digital health tools for pediatric sepsis care in LMICs. Objective: The objective of this study was to assess HCPs’ understanding, perceptions, and recommendations regarding the design and implementation of digital CDSSs for pediatric sepsis care in Bangladesh. Methods: Between February and May 2024, 18 individual semistructured in-depth interviews were conducted with HCPs (nurses and physicians) at 3 urban hospitals in Bangladesh. The data were transcribed, translated from Bangla to English, and analyzed using a framework matrix analysis approach. Participants were asked about familiarity with digital health tools, feedback on CDSS design, perceptions of the system’s utility, and barriers and facilitators to use of similar tools in clinical settings in Bangladesh. Results: Participants reported overall positive perceptions toward the potential implementation of a CDSS for pediatric sepsis care in Bangladesh. Some key priorities for the design of a CDSS were durability, re#usability, cost considerations, reliability, and accuracy. Clinicians desired the CDS tool to also have customizable alarm parameters and include additional functions such as glucose monitoring. Many favored audio (ringtone) or visual (light) alarms to alert about changes in captured vital signs. HCPs believed that a CDSS could enhance patient care by allowing greater staff capacity to monitor patients, reducing management time, and aiding in faster clinical decision-making, with some suggesting it could lower mortality rates. Concerns regarding implementation included internet availability, affordability of the wearable devices, and trust in the CDSS outputs compared to expert clinician judgement. Conclusions: The findings of this study highlight HCPs’ perceptions toward the potential of wearable biosensor devices and CDS tools (CDSSs) for improving pediatric sepsis outcomes in LMICs and highlight the need to address implementation challenges to ensure the effective integration of CDSSs into health care systems.
dlvr.it
September 26, 2025 at 12:55 PM
JMIR Formative Res: Health Care Providers’ Perspectives of Clinical Decision Support Tools for Pediatric Sepsis in Bangladesh: Qualitative Study #Sepsis #PediatricHealthcare #DigitalHealth #mHealth #ClinicalDecisionSupport
NEW: Disappearing Text as a Clinical Decision Support Layer: A Case Series www.thieme-connect.de/products/ejo...
#MedSky #CDS #ClinicalDecisionSupport #DigitalHealth
#MedSky #CDS #ClinicalDecisionSupport #DigitalHealth

September 20, 2025 at 7:35 PM
NEW: Disappearing Text as a Clinical Decision Support Layer: A Case Series www.thieme-connect.de/products/ejo...
#MedSky #CDS #ClinicalDecisionSupport #DigitalHealth
#MedSky #CDS #ClinicalDecisionSupport #DigitalHealth
ICYMI: Clinical Decision-Making and Use of Clinical Decision Support When Clinicians are Fatigued in an #EmergencyDepartment: A Qualitative Study www.thieme-connect.de/products/ejo...
#MedSky #CDS #DigitalHealth #ClinicalDecisionSupport @mozkaynak.bsky.social
#MedSky #CDS #DigitalHealth #ClinicalDecisionSupport @mozkaynak.bsky.social

September 20, 2025 at 7:32 PM
ICYMI: Clinical Decision-Making and Use of Clinical Decision Support When Clinicians are Fatigued in an #EmergencyDepartment: A Qualitative Study www.thieme-connect.de/products/ejo...
#MedSky #CDS #DigitalHealth #ClinicalDecisionSupport @mozkaynak.bsky.social
#MedSky #CDS #DigitalHealth #ClinicalDecisionSupport @mozkaynak.bsky.social
In the last three months, 𝗻𝗲𝗮𝗿𝗹𝘆 𝟭𝟬% 𝗼𝗳 𝗨.𝗦. 𝗼𝗻𝗰𝗼𝗹𝗼𝗴𝗶𝘀𝘁𝘀 signed up for our real-time Oncology library.
Hear what Dr. Peter Kaufman, Oncologist at the University of Vermont Cancer Center, had to say about Oncoscope Edge: bit.ly/41LEK6U
#Oncology #ClinicalDecisionSupport #PrecisionMedicine
Hear what Dr. Peter Kaufman, Oncologist at the University of Vermont Cancer Center, had to say about Oncoscope Edge: bit.ly/41LEK6U
#Oncology #ClinicalDecisionSupport #PrecisionMedicine

Founder Findings: How Can Oncoscope-AI Edge Help Oncology Specialists?
YouTube video by Oncoscope-AI
youtu.be
September 10, 2025 at 4:54 PM
In the last three months, 𝗻𝗲𝗮𝗿𝗹𝘆 𝟭𝟬% 𝗼𝗳 𝗨.𝗦. 𝗼𝗻𝗰𝗼𝗹𝗼𝗴𝗶𝘀𝘁𝘀 signed up for our real-time Oncology library.
Hear what Dr. Peter Kaufman, Oncologist at the University of Vermont Cancer Center, had to say about Oncoscope Edge: bit.ly/41LEK6U
#Oncology #ClinicalDecisionSupport #PrecisionMedicine
Hear what Dr. Peter Kaufman, Oncologist at the University of Vermont Cancer Center, had to say about Oncoscope Edge: bit.ly/41LEK6U
#Oncology #ClinicalDecisionSupport #PrecisionMedicine
Over half of cancers in relatives go undocumented in EHRs—risking missed chances to identify familial cancer risk and reduce preventable mortality. bit.ly/41GriRS #GIMO #FamilyHistory #CancerScreening #ElectronicHealthRecord #ClinicalDecisionSupport #Kinship

September 9, 2025 at 8:54 PM
Over half of cancers in relatives go undocumented in EHRs—risking missed chances to identify familial cancer risk and reduce preventable mortality. bit.ly/41GriRS #GIMO #FamilyHistory #CancerScreening #ElectronicHealthRecord #ClinicalDecisionSupport #Kinship
NEW: Sisyphus' Alert: The Uphill Struggle to Improve Venous #Thromboembolism Prophylaxis #ClinicalDecisionSupport www.thieme-connect.de/products/ejo...
#MedSky #CDS #DigitalHealth
#MedSky #CDS #DigitalHealth

September 6, 2025 at 8:34 PM
NEW: Sisyphus' Alert: The Uphill Struggle to Improve Venous #Thromboembolism Prophylaxis #ClinicalDecisionSupport www.thieme-connect.de/products/ejo...
#MedSky #CDS #DigitalHealth
#MedSky #CDS #DigitalHealth
JMIR Formative Res: Evaluating the Prototype of a Clinical Decision Support System in Primary Care: Qualitative Study #ClinicalDecisionSupport #PrimaryCare #HealthcareInnovation #ArtificialIntelligence #UserExperience

Evaluating the Prototype of a Clinical Decision Support System in Primary Care: Qualitative Study
Background: General practitioners are confronted with a wide variety of diseases and sometimes diagnostic uncertainty. Clinical decision support systems could be valuable to improve diagnosis, but existing tools are not adapted to the requirements and workflow in the primary setting. In the project SATURN, the prototype of a clinical decision support system based on artificial intelligence (#AI) is being developed together with users specifically for primary care in Germany. It aims to reduce diagnostic uncertainty in cases of unclear and rare diseases and focuses on three medical fields. A user-centered design approach is applied for prototype development and evaluation. Objective: This study evaluates the #usability of a high-fidelity prototype and explores aspects of user experience like the subjective impression, satisfaction and areas of improvement. Methods: Five general practitioners participated in the evaluation which consisted of (1) a remote think-aloud test, (2) a post-session interview, and (3) a survey with the System #usability Scale. During the think-aloud tests, the participants verbalized their thoughts and actions and solved several vignette based tasks. Remarkable observations were logged, transcribed with quotes, and analyzed for #usability problems and positive findings. All observations and interview responses were deductively assigned to the following categories: (1) Content, (2) Comprehensibility, (3) User-friendliness, (4) Layout, (5) Feedback, (6) Navigation. #usability problems were described in detail and solutions for improvement proposed. Median and total scores were calculated for all questionnaire items. Results: The evaluation detected both strengths and areas for improvement. The participants particularly liked the clear and well-structured layout of the prototype. Key issues identified were content-related limitations, such as the inability to enter unlisted symptoms, medications, and examination findings. Also, participants found the terminology for laboratory not suitable to their needs. Another key issue was a lack of user-friendliness concerning the time required to input medication plans and lab values. Participants expressed a need for faster data entry, potentially through direct imports from practice management systems or laboratory files. Adding symptom duration, weighting symptoms, and incorporating hereditary factors were suggestions made for improvement. Overall, the SATURN prototype was deemed useful and promising for future clinical use, despite the need for further refinements, particularly in the areas of data entry, as this is a key obstacle to its use. Conclusions: The #usability evaluation methods combined proved to be location independent and easy to use. They provided important findings on #usability issues and improvements that will be implemented in a second high-fidelity prototype, which will also be tested by users. Technically demanding user requirements, such as direct data transfer from the practice management system and entry options that require complex data models were beyond the scope of this project, but should be considered in future development projects.
dlvr.it
August 21, 2025 at 1:05 AM
JMIR Formative Res: Evaluating the Prototype of a Clinical Decision Support System in Primary Care: Qualitative Study #ClinicalDecisionSupport #PrimaryCare #HealthcareInnovation #ArtificialIntelligence #UserExperience
Comparison of OneChoice(R) AI-based clinical decision support recommendations with infectious disease specialists and non-specialists for bacteremia treatment in Lima, Peru
Caceres, J., Chavez-Lencinas, C. et al.
Paper
Details
#OneChoiceAI #ClinicalDecisionSupport #BacteremiaTreatmentPeru
Caceres, J., Chavez-Lencinas, C. et al.
Paper
Details
#OneChoiceAI #ClinicalDecisionSupport #BacteremiaTreatmentPeru
August 18, 2025 at 4:01 PM
Comparison of OneChoice(R) AI-based clinical decision support recommendations with infectious disease specialists and non-specialists for bacteremia treatment in Lima, Peru
Caceres, J., Chavez-Lencinas, C. et al.
Paper
Details
#OneChoiceAI #ClinicalDecisionSupport #BacteremiaTreatmentPeru
Caceres, J., Chavez-Lencinas, C. et al.
Paper
Details
#OneChoiceAI #ClinicalDecisionSupport #BacteremiaTreatmentPeru
New in JMIR Nursing: Development of a Knowledge Base for an Integrated Older Adult Care Model (SMART System) Based on an Intervention Mapping Framework: Mixed Methods Study #ElderlyCare #MobileHealth #HealthcareInnovation #IoT #ClinicalDecisionSupport

Development of a Knowledge Base for an Integrated Older Adult Care Model (SMART System) Based on an Intervention Mapping Framework: Mixed Methods Study
Background: Although mobile health applications integrated with Internet of Things-enabled devices are increasingly used to satisfy the growing needs for home-based elderly care resulting from rapid population aging, their effectiveness is constrained by three key challenges: a focus on specific functions rather than holistic and integrated support, absence of a solid theoretical framework for development, and a lack of personalized, real-time feedback to address diverse care needs. To overcome these limitations, we developed a knowledge-based Clinical Decision Support System using mobile health technology – an Intelligent and Integrated Elderly Care Model (SMART system). Objective: This study aims to systematically outline the development process and outcomes of a knowledge base and trigger rules for the SMART system. Methods: Our study adopted a user-centered approach guided by the #nursing process and Intervention Mapping (IM) framework. We first identified elderly care needs through semi-structured in-depth interviews. Guided by the #nursing process and informed by guidance from the World Health Organization’s Integrated Care for Older People and WHO International Classification of Functioning, Disability, and Health, along with the North American Nursing Diagnosis Association-I #nursing diagnosis, we then determined care problems along with their underlying causes and/or risk factors and diagnostic criteria. Building on these findings, we applied the first three steps of the IM framework to formulate corresponding long-term and short-term care objectives, select appropriate evidence-based interventions, and match practical implementation approaches, which were grounded in rigorous evidence derived from systematic literature reviews, clinical guidelines, and expert insights. We also developed a set of trigger rules to link abnormalities in elderly individuals with corresponding care problems and interventions in the SMART knowledge base. Results: The semi-structured in-depth interviews identified five types of care needs: daily life care, healthcare, external support, social participation, and self-development, which formed the foundation of the SMART knowledge base. Based on this, we identified 138 care problems, each with associated causes and/or risk factors and diagnostic criteria. The objective matrix comprised 138 long-term and 195 short-term care objectives. Guided by 15 expert-defined selection criteria, we then selected 450 evidence-based interventions, each paired with at least one feasible and practical implementation approach. Additionally, we developed diagnostic rules to match the assessment data with relevant care problems and their causes and/or risk factors, and intervention trigger rules to formulate personalized interventions based on individual characteristics, ensuring tailored care aligned with specific care objectives. Conclusions: This study outlines the development process and outcomes of the SMART knowledge base and trigger rules. The study methodology offers theoretical support for developing knowledge bases and trigger rules of similar Clinical Decision Support Systems for home-based elderly care.
dlvr.it
August 14, 2025 at 11:08 PM
New in JMIR Nursing: Development of a Knowledge Base for an Integrated Older Adult Care Model (SMART System) Based on an Intervention Mapping Framework: Mixed Methods Study #ElderlyCare #MobileHealth #HealthcareInnovation #IoT #ClinicalDecisionSupport
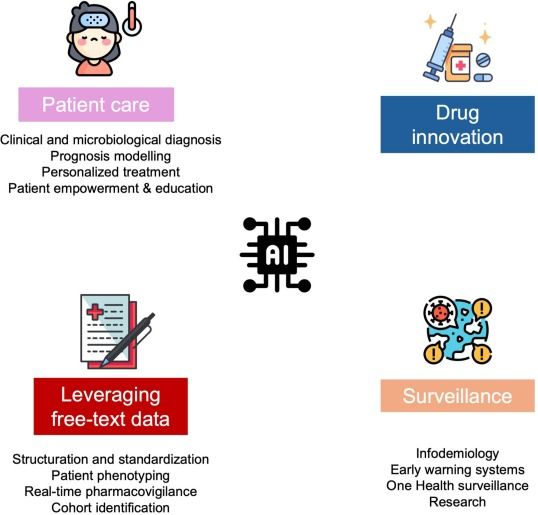
[Publication] The article "Artificial intelligence and infectious diseases: Scope and perspectives" is now available.
www.sciencedirect.com/science/arti...
#IDsky #InfectiousDiseases #ArtificialIntelligence #GenerativeArtificialIntelligence #MachineLearning #ClinicalDecisionSupport
www.sciencedirect.com/science/arti...
#IDsky #InfectiousDiseases #ArtificialIntelligence #GenerativeArtificialIntelligence #MachineLearning #ClinicalDecisionSupport

Artificial intelligence and infectious diseases: Scope and perspectives
Artificial intelligence (AI) is set to permeate every facet of infectious disease practice—from prevention and public health surveillance to epidemic …
www.sciencedirect.com
August 6, 2025 at 7:29 AM
[Publication] The article "Artificial intelligence and infectious diseases: Scope and perspectives" is now available.
www.sciencedirect.com/science/arti...
#IDsky #InfectiousDiseases #ArtificialIntelligence #GenerativeArtificialIntelligence #MachineLearning #ClinicalDecisionSupport
www.sciencedirect.com/science/arti...
#IDsky #InfectiousDiseases #ArtificialIntelligence #GenerativeArtificialIntelligence #MachineLearning #ClinicalDecisionSupport

My latest blog post on the importance of language in the age of medical #AI #LLM and #clinicaldecisionsupport Watch your commas, people!
venturevalkyrie.com/ai-large-lan...
venturevalkyrie.com/ai-large-lan...
AI, Large Language Models and How a Comma Could Actually Kill You
venturevalkyrie.com
July 13, 2025 at 3:54 AM
My latest blog post on the importance of language in the age of medical #AI #LLM and #clinicaldecisionsupport Watch your commas, people!
venturevalkyrie.com/ai-large-lan...
venturevalkyrie.com/ai-large-lan...

🦿 There are over 200 #ProstheticFeet on the market.
But patients rarely have the opportunity to trial different options. Caplex™️ changes that.
Experience multiple options in a single session—and walk away with the one that works best for them.
🔗 humotech.com/clinical/
#ClinicalDecisionSupport
But patients rarely have the opportunity to trial different options. Caplex™️ changes that.
Experience multiple options in a single session—and walk away with the one that works best for them.
🔗 humotech.com/clinical/
#ClinicalDecisionSupport

June 25, 2025 at 2:04 PM
🦿 There are over 200 #ProstheticFeet on the market.
But patients rarely have the opportunity to trial different options. Caplex™️ changes that.
Experience multiple options in a single session—and walk away with the one that works best for them.
🔗 humotech.com/clinical/
#ClinicalDecisionSupport
But patients rarely have the opportunity to trial different options. Caplex™️ changes that.
Experience multiple options in a single session—and walk away with the one that works best for them.
🔗 humotech.com/clinical/
#ClinicalDecisionSupport
📢 Stay tuned — we’ll be sharing key takeaways and insights from the workshop in the coming weeks!
#PERMANENS #IASP2025 #MentalHealth #SuicidePrevention #ClinicalDecisionSupport #SelfHarm #DigitalHealth #EmergencyCare
#PERMANENS #IASP2025 #MentalHealth #SuicidePrevention #ClinicalDecisionSupport #SelfHarm #DigitalHealth #EmergencyCare
June 20, 2025 at 9:13 AM
📢 Stay tuned — we’ll be sharing key takeaways and insights from the workshop in the coming weeks!
#PERMANENS #IASP2025 #MentalHealth #SuicidePrevention #ClinicalDecisionSupport #SelfHarm #DigitalHealth #EmergencyCare
#PERMANENS #IASP2025 #MentalHealth #SuicidePrevention #ClinicalDecisionSupport #SelfHarm #DigitalHealth #EmergencyCare