



Rémi Goupil
@goupilremi.bsky.social
Nephrologist and FRQS clinician-scientist in hypertension at the Hôpital du Sacré-Coeur de Montréal. Associate Clinical Prof at Université de Montréal. Proud father of four.
Reposted by Rémi Goupil

Please fill out this 10-minute survey from colleagues of Hypertension Canada on the standardized BP procedure.
redcap.link/barriers.to....
Feel free to fill out a survey for each clinical site where you measure BP in an outpatient setting.
redcap.link/barriers.to....
Feel free to fill out a survey for each clinical site where you measure BP in an outpatient setting.
Language
redcap.link
October 23, 2025 at 10:21 AM
Please fill out this 10-minute survey from colleagues of Hypertension Canada on the standardized BP procedure.
redcap.link/barriers.to....
Feel free to fill out a survey for each clinical site where you measure BP in an outpatient setting.
redcap.link/barriers.to....
Feel free to fill out a survey for each clinical site where you measure BP in an outpatient setting.
Reposted by Rémi Goupil

Subclinical primary aldosteronism is an under-recognized driver of cardiovascular risk. Could it be a new target for CV prevention? Read our Circulation editorial —>
September 29, 2025 at 7:03 PM
Subclinical primary aldosteronism is an under-recognized driver of cardiovascular risk. Could it be a new target for CV prevention? Read our Circulation editorial —>
Reposted by Rémi Goupil

Such a great opportunity, to be involved in an editorial on the most recent evidence for Subclinical Primary Aldosteronism. Thank you to @drwanpen.bsky.social @giaconajohn.bsky.social
Go check it out!! www.ahajournals.org/doi/10.1161/...
Go check it out!! www.ahajournals.org/doi/10.1161/...

September 29, 2025 at 6:52 PM
Such a great opportunity, to be involved in an editorial on the most recent evidence for Subclinical Primary Aldosteronism. Thank you to @drwanpen.bsky.social @giaconajohn.bsky.social
Go check it out!! www.ahajournals.org/doi/10.1161/...
Go check it out!! www.ahajournals.org/doi/10.1161/...
Reposted by Rémi Goupil

Doesn’t take too long!
All those who think it is hard to measure BP properly in the clinic please fill out this survey from @goupilremi.bsky.social
#NephSky #CardioSky #MedSky
All those who think it is hard to measure BP properly in the clinic please fill out this survey from @goupilremi.bsky.social
#NephSky #CardioSky #MedSky
🚨 Survey Alert!
Standardized office BP measurements are recommended everywhere, but still underused.
We want to hear from you: what are the barriers to using them as a routine in clinical practice?
Click here to read the consent form and take the survey:
redcap.link/barriers.to....
Standardized office BP measurements are recommended everywhere, but still underused.
We want to hear from you: what are the barriers to using them as a routine in clinical practice?
Click here to read the consent form and take the survey:
redcap.link/barriers.to....
September 22, 2025 at 10:20 PM
Doesn’t take too long!
All those who think it is hard to measure BP properly in the clinic please fill out this survey from @goupilremi.bsky.social
#NephSky #CardioSky #MedSky
All those who think it is hard to measure BP properly in the clinic please fill out this survey from @goupilremi.bsky.social
#NephSky #CardioSky #MedSky
🚨 Survey Alert!
Standardized office BP measurements are recommended everywhere, but still underused.
We want to hear from you: what are the barriers to using them as a routine in clinical practice?
Click here to read the consent form and take the survey:
redcap.link/barriers.to....
Standardized office BP measurements are recommended everywhere, but still underused.
We want to hear from you: what are the barriers to using them as a routine in clinical practice?
Click here to read the consent form and take the survey:
redcap.link/barriers.to....
September 22, 2025 at 4:19 PM
🚨 Survey Alert!
Standardized office BP measurements are recommended everywhere, but still underused.
We want to hear from you: what are the barriers to using them as a routine in clinical practice?
Click here to read the consent form and take the survey:
redcap.link/barriers.to....
Standardized office BP measurements are recommended everywhere, but still underused.
We want to hear from you: what are the barriers to using them as a routine in clinical practice?
Click here to read the consent form and take the survey:
redcap.link/barriers.to....
Reposted by Rémi Goupil
Another great read on implementation of the new BP guidelines:
Implementing the 2025 Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: How to Translate Team-Based Care of Hypertension to the Real World www.ahajournals.org/doi/10.1161/...
Implementing the 2025 Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: How to Translate Team-Based Care of Hypertension to the Real World www.ahajournals.org/doi/10.1161/...
American Heart Association Journals
www.ahajournals.org
August 15, 2025 at 10:08 AM
Another great read on implementation of the new BP guidelines:
Implementing the 2025 Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: How to Translate Team-Based Care of Hypertension to the Real World www.ahajournals.org/doi/10.1161/...
Implementing the 2025 Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: How to Translate Team-Based Care of Hypertension to the Real World www.ahajournals.org/doi/10.1161/...
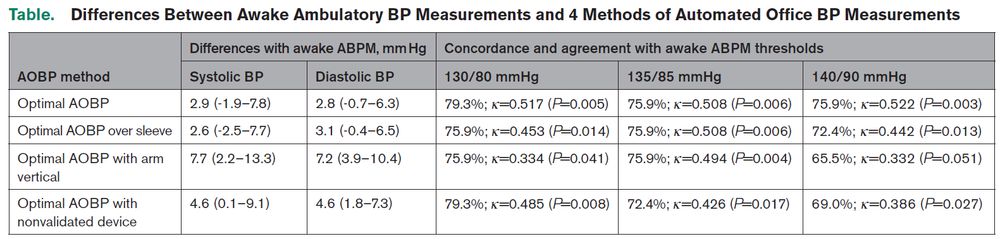
Just published in Hypertension! In a pilot study, we tested whether common "shortcuts" of the standardized AOBP measurement procedure affect accuracy, assessed with daytime ABPM.
www.ahajournals.org/doi/10.1161/...
www.ahajournals.org/doi/10.1161/...

Simplifications of the Standardized BP Measurement Procedure and Accuracy: The SIMPLE-AOBP Randomized Cross-Over Trial | Hypertension
www.ahajournals.org
July 17, 2025 at 6:10 PM
Just published in Hypertension! In a pilot study, we tested whether common "shortcuts" of the standardized AOBP measurement procedure affect accuracy, assessed with daytime ABPM.
www.ahajournals.org/doi/10.1161/...
www.ahajournals.org/doi/10.1161/...
Reposted by Rémi Goupil
Cool trial (thx Dr. Cluett for sharing!). I love the within person comparison.
@goupilremi.bsky.social @deanpicone.bsky.social
Random ? (having enjoyed reading & doing similar studies): Is accuracy at a single time enough? Should we worry about BP change too?
www.ahajournals.org/doi/10.1161/...
@goupilremi.bsky.social @deanpicone.bsky.social
Random ? (having enjoyed reading & doing similar studies): Is accuracy at a single time enough? Should we worry about BP change too?
www.ahajournals.org/doi/10.1161/...
July 17, 2025 at 2:03 PM
Cool trial (thx Dr. Cluett for sharing!). I love the within person comparison.
@goupilremi.bsky.social @deanpicone.bsky.social
Random ? (having enjoyed reading & doing similar studies): Is accuracy at a single time enough? Should we worry about BP change too?
www.ahajournals.org/doi/10.1161/...
@goupilremi.bsky.social @deanpicone.bsky.social
Random ? (having enjoyed reading & doing similar studies): Is accuracy at a single time enough? Should we worry about BP change too?
www.ahajournals.org/doi/10.1161/...
Our new data on subclinical PA and MACE is out in Circulation! For the first time, we show that renin-independant aldosterone production is associated with an increased risk of MACE independently of BP, in people mostly normotensive with low CV risk.
www.ahajournals.org/doi/full/10....
www.ahajournals.org/doi/full/10....
July 10, 2025 at 7:21 PM
Our new data on subclinical PA and MACE is out in Circulation! For the first time, we show that renin-independant aldosterone production is associated with an increased risk of MACE independently of BP, in people mostly normotensive with low CV risk.
www.ahajournals.org/doi/full/10....
www.ahajournals.org/doi/full/10....
Aujourd’hui est un grand jour! Publication, pour la première fois, des lignes directrices d’Hypertension Canada en français! Merci à la Société québécoise d’hypertension artérielle pour le soutien à la traduction du guide et de ses annexes!
www.cmaj.ca/content/197/...
www.cmaj.ca/content/197/...

Guide de pratique clinique en soins de première ligne d’Hypertension Canada pour le diagnostic et le traitement de l’hypertension artérielle chez les adultes
Contexte: Le Canada a longtemps figuré parmi les leaders mondiaux de la prise en charge de l’hypertension artérielle (HTA), mais ses taux de traitement et de maîtrise de l’HTA ont régressé ces dernièr...
www.cmaj.ca
June 16, 2025 at 1:37 PM
Aujourd’hui est un grand jour! Publication, pour la première fois, des lignes directrices d’Hypertension Canada en français! Merci à la Société québécoise d’hypertension artérielle pour le soutien à la traduction du guide et de ses annexes!
www.cmaj.ca/content/197/...
www.cmaj.ca/content/197/...
Reposted by Rémi Goupil

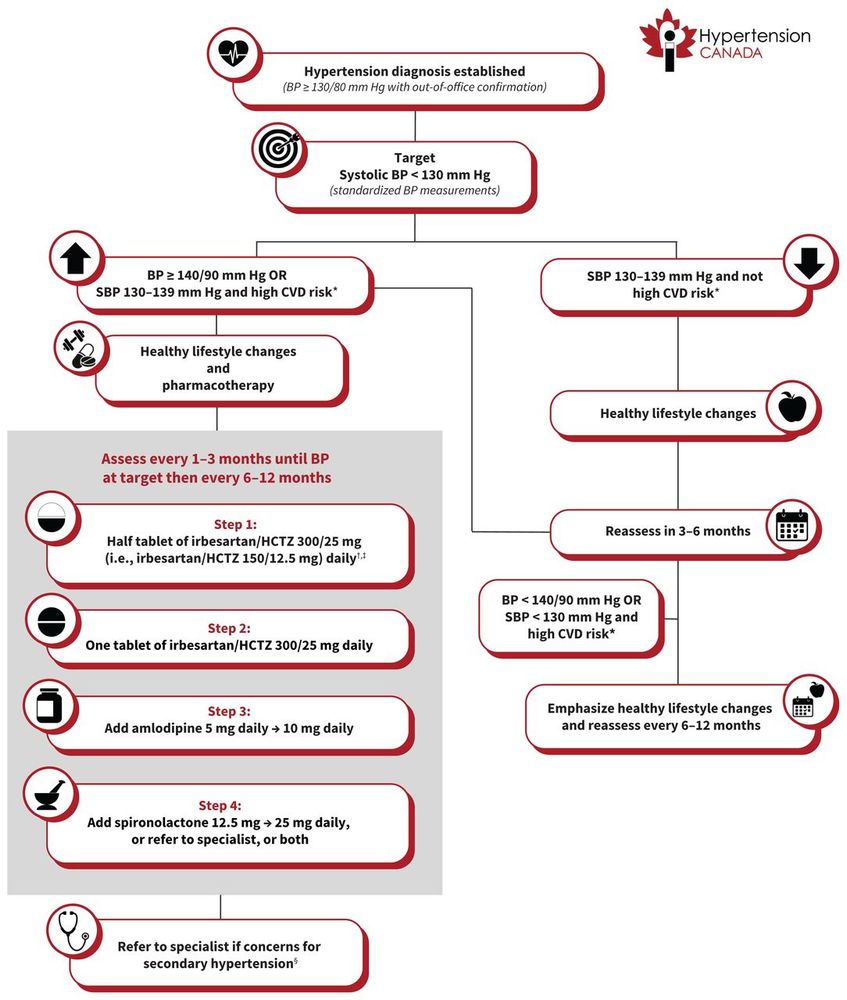
A new era in hypertension management-Simplified and practical guidelines. Here is what you need to know: 130/80mmHg and ARB-diuretic combination.
May 27, 2025 at 12:51 AM
A new era in hypertension management-Simplified and practical guidelines. Here is what you need to know: 130/80mmHg and ARB-diuretic combination.
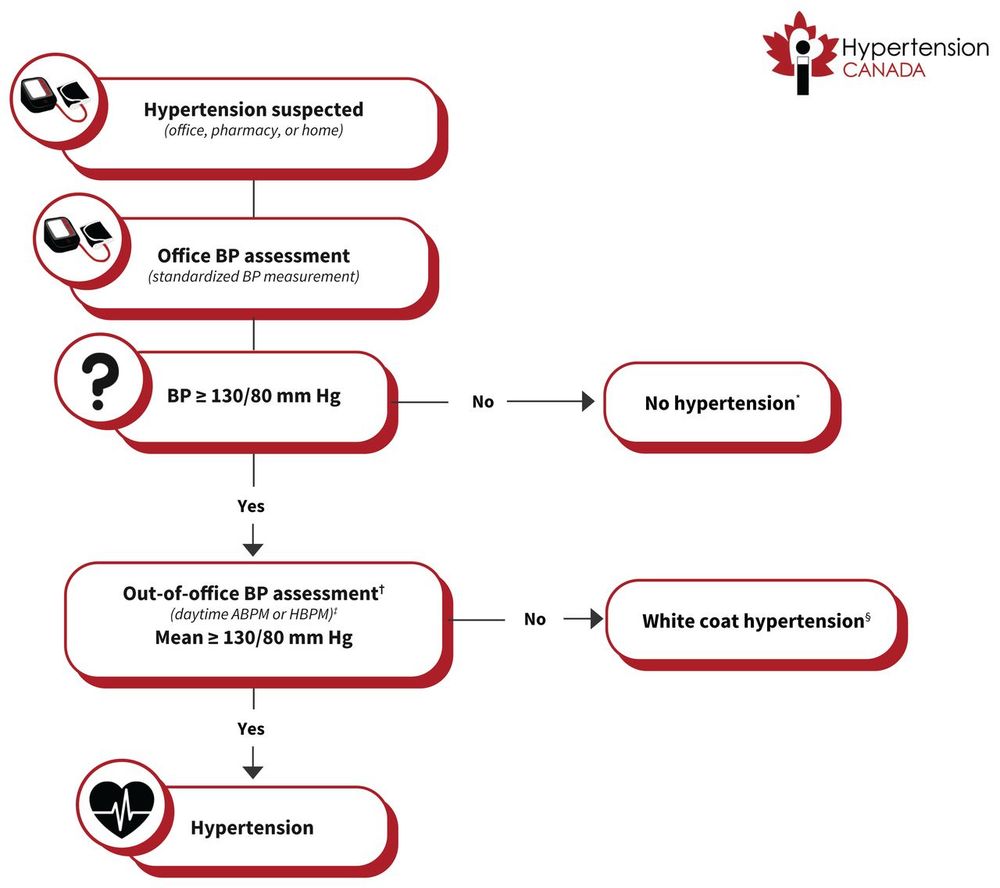
The new Hypertension Canada guideline is out today! Designed for and by Primary care to provide pragmatic and easy to implement recommendations to improve hypertension care in adults in Canada. @hypertensioncanada.bsky.social @cmaj.bsky.social www.cmaj.ca/content/197/...

Hypertension Canada guideline for the diagnosis and treatment of hypertension in adults in primary care
Background: Canada has historically been among the world leaders in hypertension care, but hypertension treatment and control rates have regressed in recent years. This guideline is intended to provid...
www.cmaj.ca
May 26, 2025 at 1:31 PM
The new Hypertension Canada guideline is out today! Designed for and by Primary care to provide pragmatic and easy to implement recommendations to improve hypertension care in adults in Canada. @hypertensioncanada.bsky.social @cmaj.bsky.social www.cmaj.ca/content/197/...
Reposted by Rémi Goupil
The new @hypertensioncanada.bsky.social guidelines are live at @cmaj.ca www.cmaj.ca/content/197/...
130/80 for everyone?
#Hypertension
130/80 for everyone?
#Hypertension

Hypertension Canada guideline for the diagnosis and treatment of hypertension in adults in primary care
Background: Canada has historically been among the world leaders in hypertension care, but hypertension treatment and control rates have regressed in recent years. This guideline is intended to provid...
www.cmaj.ca
May 26, 2025 at 10:21 AM
The new @hypertensioncanada.bsky.social guidelines are live at @cmaj.ca www.cmaj.ca/content/197/...
130/80 for everyone?
#Hypertension
130/80 for everyone?
#Hypertension
Reposted by Rémi Goupil

June 5 - 2025 Primary Care Guidelines Webinar
us06web.zoom.us/webinar/regi...
June 12 - Lignes directrices 2025 d'Hypertension Canada
us06web.zoom.us/webinar/regi...
us06web.zoom.us/webinar/regi...
June 12 - Lignes directrices 2025 d'Hypertension Canada
us06web.zoom.us/webinar/regi...


May 8, 2025 at 4:35 PM
June 5 - 2025 Primary Care Guidelines Webinar
us06web.zoom.us/webinar/regi...
June 12 - Lignes directrices 2025 d'Hypertension Canada
us06web.zoom.us/webinar/regi...
us06web.zoom.us/webinar/regi...
June 12 - Lignes directrices 2025 d'Hypertension Canada
us06web.zoom.us/webinar/regi...
All Canadians, please take the time to fill out this survey. It will help us identify the most important topics for our next comprehensive hypertension guideline.
There is still time to have your say!
Hypertension Canada is commencing the process of updating its comprehensive hypertension guideline. We invite you to participate in determining the priority of topics to be addressed by completing the survey.
forms.office.com/pages/respon...
Hypertension Canada is commencing the process of updating its comprehensive hypertension guideline. We invite you to participate in determining the priority of topics to be addressed by completing the survey.
forms.office.com/pages/respon...
Microsoft Forms
forms.office.com
April 9, 2025 at 7:22 PM
All Canadians, please take the time to fill out this survey. It will help us identify the most important topics for our next comprehensive hypertension guideline.
Reposted by Rémi Goupil
Have your say!
Hypertension Canada is commencing the process of updating its comprehensive hypertension guideline. We invite you to participate in determining the priority of topics to be addressed by completing the survey.
forms.office.com/pages/respon...
Hypertension Canada is commencing the process of updating its comprehensive hypertension guideline. We invite you to participate in determining the priority of topics to be addressed by completing the survey.
forms.office.com/pages/respon...
Microsoft Forms
forms.office.com
March 26, 2025 at 8:30 PM
Have your say!
Hypertension Canada is commencing the process of updating its comprehensive hypertension guideline. We invite you to participate in determining the priority of topics to be addressed by completing the survey.
forms.office.com/pages/respon...
Hypertension Canada is commencing the process of updating its comprehensive hypertension guideline. We invite you to participate in determining the priority of topics to be addressed by completing the survey.
forms.office.com/pages/respon...
Reposted by Rémi Goupil
The Hypertension Canada statement on #cuffless BP is available at @amjhypertension.bsky.social
academic.oup.com/ajh/advance-...
lead by @goupilremi.bsky.social and Cederick Landry
As you can see we discuss the technology but are not enthused about what we have seen so far
#Hypertension
academic.oup.com/ajh/advance-...
lead by @goupilremi.bsky.social and Cederick Landry
As you can see we discuss the technology but are not enthused about what we have seen so far
#Hypertension

January 8, 2025 at 12:27 AM
The Hypertension Canada statement on #cuffless BP is available at @amjhypertension.bsky.social
academic.oup.com/ajh/advance-...
lead by @goupilremi.bsky.social and Cederick Landry
As you can see we discuss the technology but are not enthused about what we have seen so far
#Hypertension
academic.oup.com/ajh/advance-...
lead by @goupilremi.bsky.social and Cederick Landry
As you can see we discuss the technology but are not enthused about what we have seen so far
#Hypertension
I might as well start with this as a first post! Hypertension Canada is hard at work to publish new guidelines. Our first step, guidelines based on WHO’s HEARTS initiative made for and by Primary Care will soon be submitted for publication. See this for details: onlinecjc.ca/article/S082...

Ushering in a New Era of Hypertension Canada Guidelines: A Roadmap of What Lies Ahead
Hypertension is a global health problem with an estimated prevalence of 32% worldwide
and rising.1 In fact, hypertension is the most common modifiable risk factor for cardiovascular
disease and mortal...
onlinecjc.ca
November 13, 2024 at 4:14 AM
I might as well start with this as a first post! Hypertension Canada is hard at work to publish new guidelines. Our first step, guidelines based on WHO’s HEARTS initiative made for and by Primary Care will soon be submitted for publication. See this for details: onlinecjc.ca/article/S082...