



James Greenan-Barrett
@jgreenanbarrett.bsky.social
NIHR Academic Clinical Fellow in Infectious Diseases | Specialist Registrar in Infectious Diseases & General Internal Medicine | UCL Respiratory & LSHTM | Interested in TB biomarkers, disease states & natural history
Reposted by James Greenan-Barrett
Check out our new paper in @lancetmicrobe.bsky.social
In this IPD-MA we show that single-gene transcripts are equivalent to multi-gene signatures to Dx subclinical TB
They perform consistently across settings + show potential clinical utility to stratify therapy
#IDsky #TBsky
bit.ly/47jU7GN
In this IPD-MA we show that single-gene transcripts are equivalent to multi-gene signatures to Dx subclinical TB
They perform consistently across settings + show potential clinical utility to stratify therapy
#IDsky #TBsky
bit.ly/47jU7GN

Single-gene transcripts for subclinical tuberculosis: an individual participant data meta-analysis
Single-gene transcripts are equivalent to multi-gene signatures for detection of subclinical
tuberculosis, with consistent performance across settings. Single-gene transcripts
show potential clinical ...
bit.ly
October 14, 2025 at 11:31 AM
Check out our new paper in @lancetmicrobe.bsky.social
In this IPD-MA we show that single-gene transcripts are equivalent to multi-gene signatures to Dx subclinical TB
They perform consistently across settings + show potential clinical utility to stratify therapy
#IDsky #TBsky
bit.ly/47jU7GN
In this IPD-MA we show that single-gene transcripts are equivalent to multi-gene signatures to Dx subclinical TB
They perform consistently across settings + show potential clinical utility to stratify therapy
#IDsky #TBsky
bit.ly/47jU7GN
Check out our new paper in @lancetmicrobe.bsky.social
In this IPD-MA we show that single-gene transcripts are equivalent to multi-gene signatures to Dx subclinical TB
They perform consistently across settings + show potential clinical utility to stratify therapy
#IDsky #TBsky
bit.ly/47jU7GN
In this IPD-MA we show that single-gene transcripts are equivalent to multi-gene signatures to Dx subclinical TB
They perform consistently across settings + show potential clinical utility to stratify therapy
#IDsky #TBsky
bit.ly/47jU7GN
Single-gene transcripts for subclinical tuberculosis: an individual participant data meta-analysis
Single-gene transcripts are equivalent to multi-gene signatures for detection of subclinical
tuberculosis, with consistent performance across settings. Single-gene transcripts
show potential clinical ...
bit.ly
October 14, 2025 at 11:31 AM
Check out our new paper in @lancetmicrobe.bsky.social
In this IPD-MA we show that single-gene transcripts are equivalent to multi-gene signatures to Dx subclinical TB
They perform consistently across settings + show potential clinical utility to stratify therapy
#IDsky #TBsky
bit.ly/47jU7GN
In this IPD-MA we show that single-gene transcripts are equivalent to multi-gene signatures to Dx subclinical TB
They perform consistently across settings + show potential clinical utility to stratify therapy
#IDsky #TBsky
bit.ly/47jU7GN
Reposted by James Greenan-Barrett

Optimising the use of currently available treatments through treatment stratification could reduce treatment duration by 2-months for the majority. TB treatment stratification strategies should be prospectively trialled in a phase III RCT.
#TBSky
#TBSky
June 13, 2025 at 8:25 AM
Optimising the use of currently available treatments through treatment stratification could reduce treatment duration by 2-months for the majority. TB treatment stratification strategies should be prospectively trialled in a phase III RCT.
#TBSky
#TBSky
Reposted by James Greenan-Barrett

We’re hiring! Looking for a laboratory post-doc fellow to help us disentangle protective and pathogenic T cells in TB, so we can stratify disease-risk after infection, and develop more effective vaccines. Interdisciplinary science in the heart of London. What's not to like? More here: bit.ly/4iIEiwu

March 27, 2025 at 10:58 PM
We’re hiring! Looking for a laboratory post-doc fellow to help us disentangle protective and pathogenic T cells in TB, so we can stratify disease-risk after infection, and develop more effective vaccines. Interdisciplinary science in the heart of London. What's not to like? More here: bit.ly/4iIEiwu
Reposted by James Greenan-Barrett

New preprint (with all pre-print caveats!) tinyurl.com/589ffhu4 on Mtb infection risk by sex & age.
Men are at higher risk of #tuberculosis v women- but unclear how much driven by higher infection vs progression to disease. We meta-analysed Mtb immunoreactivity surveys to find out more🧵 #tbsky
Men are at higher risk of #tuberculosis v women- but unclear how much driven by higher infection vs progression to disease. We meta-analysed Mtb immunoreactivity surveys to find out more🧵 #tbsky
Sex Differences in the Risk of Mycobacterium Tuberculosis Infection: A Systematic Review and Meta-Analysis of Population-Based Immunoreactivity Surveys
Background: Tuberculosis (TB) killed 1·25 million people globally in 2023. Men have a 1·7-fold higher TB incidence than women, but it is not known to what exten
papers.ssrn.com
January 10, 2025 at 8:20 AM
New preprint (with all pre-print caveats!) tinyurl.com/589ffhu4 on Mtb infection risk by sex & age.
Men are at higher risk of #tuberculosis v women- but unclear how much driven by higher infection vs progression to disease. We meta-analysed Mtb immunoreactivity surveys to find out more🧵 #tbsky
Men are at higher risk of #tuberculosis v women- but unclear how much driven by higher infection vs progression to disease. We meta-analysed Mtb immunoreactivity surveys to find out more🧵 #tbsky
“…despite the recent introduction of BPaL/M, resistance to these new antituberculosis drugs has already developed in at least 27 countries across four continents. Furthermore, a quarter of these cases involved patient-to-patient transmission”
Worrying stuff
Worrying stuff

⚠️ Bit of an alarm bell to MDR-TB regimen BPaL/M - resistance to constituent antibiotics developing and transmission of such strains already occurring
#TBSky #IDSky @nejm.org
www.nejm.org/doi/10.1056/...
#TBSky #IDSky @nejm.org
www.nejm.org/doi/10.1056/...
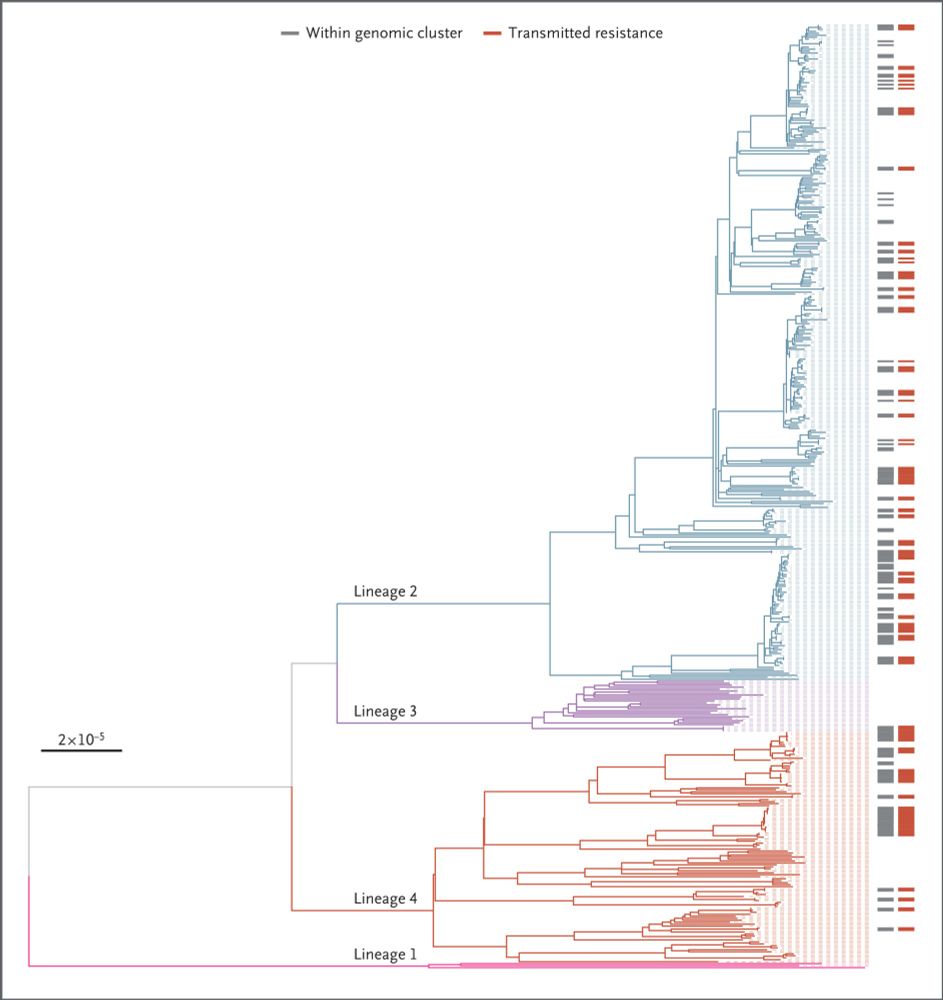
Transmission as a Key Driver of Resistance to the New Tuberculosis Drugs | NEJM
Whole-genome sequencing was used to show that resistance to newer antituberculosis
drugs is present in at least 27 countries and that up to a quarter of this resistance
may be due to person-to-...
www.nejm.org
January 5, 2025 at 8:27 AM
“…despite the recent introduction of BPaL/M, resistance to these new antituberculosis drugs has already developed in at least 27 countries across four continents. Furthermore, a quarter of these cases involved patient-to-patient transmission”
Worrying stuff
Worrying stuff
Reposted by James Greenan-Barrett

Interested in the immunopathology of human tuberculosis? Here is our latest review:
www.science.org/doi/10.1126/...
www.science.org/doi/10.1126/...

Immunopathology in human tuberculosis
The balance between protective and pathological immune responses shapes progression of Mycobacterium tuberculosis infection.
www.science.org
December 13, 2024 at 10:59 PM
Interested in the immunopathology of human tuberculosis? Here is our latest review:
www.science.org/doi/10.1126/...
www.science.org/doi/10.1126/...
Reposted by James Greenan-Barrett

🆕️⚡️⚡️Selected TB blood RNA signatures& CRP do not provide biomarkers of microbiological clearance to support TB treatment cessation at 8 weeks
CRP achieved marginal albeit statistically significant discrimination/AUROC 0.69(95%CI 0.52–0.87) #idsky #medsky #tbsky
publications.ersnet.org/content/erj/...
CRP achieved marginal albeit statistically significant discrimination/AUROC 0.69(95%CI 0.52–0.87) #idsky #medsky #tbsky
publications.ersnet.org/content/erj/...

November 21, 2024 at 1:40 PM
🆕️⚡️⚡️Selected TB blood RNA signatures& CRP do not provide biomarkers of microbiological clearance to support TB treatment cessation at 8 weeks
CRP achieved marginal albeit statistically significant discrimination/AUROC 0.69(95%CI 0.52–0.87) #idsky #medsky #tbsky
publications.ersnet.org/content/erj/...
CRP achieved marginal albeit statistically significant discrimination/AUROC 0.69(95%CI 0.52–0.87) #idsky #medsky #tbsky
publications.ersnet.org/content/erj/...
Reposted by James Greenan-Barrett
First wave ISGs (eg MX1) induced rapidly, correlate with VL & infectivity - potential biomarker to stratify patients who'll benefit from antivirals?

November 30, 2024 at 2:50 PM
First wave ISGs (eg MX1) induced rapidly, correlate with VL & infectivity - potential biomarker to stratify patients who'll benefit from antivirals?
Check out our paper on RNA biomarkers in COVID-19
MX1 expression occurred early in infection before PCR detection…potential role to stratify treatment
#IDSky
MX1 expression occurred early in infection before PCR detection…potential role to stratify treatment
#IDSky
Also out now.. after peer review, our analysis of blood transcriptional biomarkers of acute respiratory viral infection leveraging the SARS-CoV-2 human challenge model: www.nature.com/articles/s41...
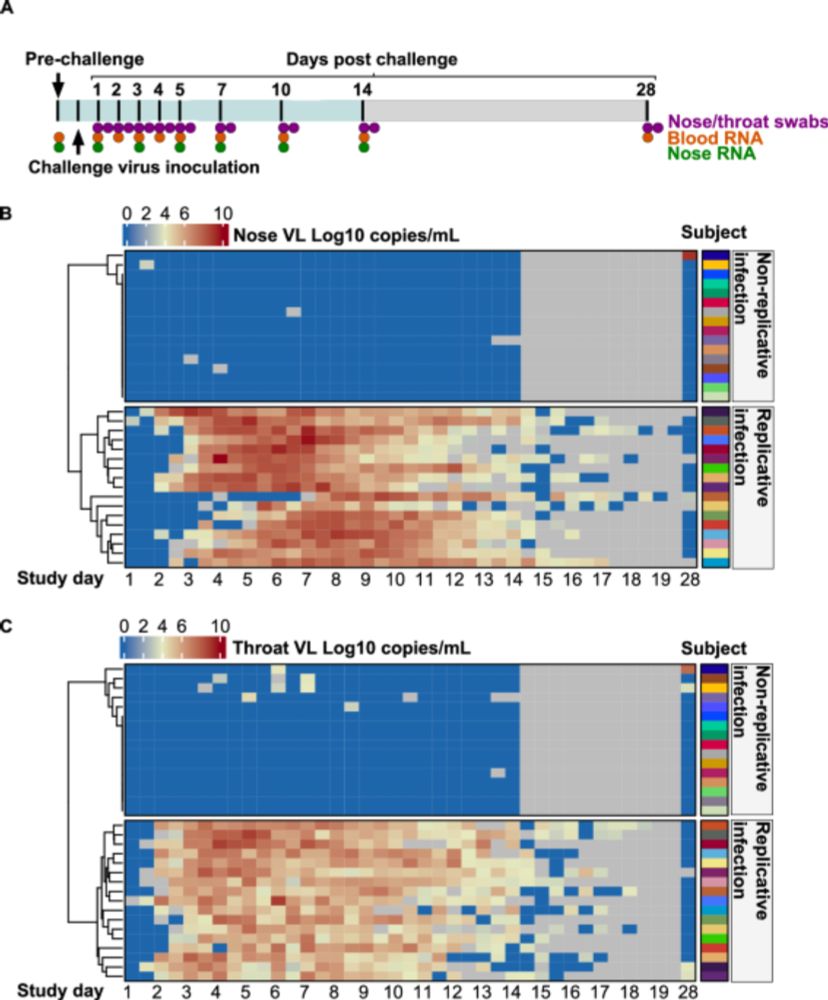
SARS-CoV-2 human challenge reveals biomarkers that discriminate early and late phases of respiratory viral infections - Nature Communications
It’s not always clear whether blood biomarkers are differentially expressed in the time course of viral infections. In this SARS-CoV-2 human challenge study, the authors identify distinct single-gene ...
www.nature.com
December 1, 2024 at 10:21 PM
Check out our paper on RNA biomarkers in COVID-19
MX1 expression occurred early in infection before PCR detection…potential role to stratify treatment
#IDSky
MX1 expression occurred early in infection before PCR detection…potential role to stratify treatment
#IDSky
Historical evidence that mass CXR screening is feasible and effective
Very cool study - lots to be learnt from the past…
#TBSky
Very cool study - lots to be learnt from the past…
#TBSky

DYK in 1957, Glasgow, Scotland ran the largest ever screening campaign against #tuberculosis?
715,000 people (76% of entire adult population) were X-rayed over just 5 weeks!
In a new study, we looked at the long-term impact of this campaign. journals.plos.org/plosmedicine...
#episky #idsky 🧪🛟
715,000 people (76% of entire adult population) were X-rayed over just 5 weeks!
In a new study, we looked at the long-term impact of this campaign. journals.plos.org/plosmedicine...
#episky #idsky 🧪🛟

November 19, 2024 at 11:21 PM
Historical evidence that mass CXR screening is feasible and effective
Very cool study - lots to be learnt from the past…
#TBSky
Very cool study - lots to be learnt from the past…
#TBSky
#UnionConf2024 has wrapped up, and what a conference! Some fascinating talks and great discussions. Seems to me that there are more questions than answers right now in #TBSky but its an exciting time..
Some personal highlights (in no particular order):
1/10
Some personal highlights (in no particular order):
1/10
November 18, 2024 at 11:06 AM
#UnionConf2024 has wrapped up, and what a conference! Some fascinating talks and great discussions. Seems to me that there are more questions than answers right now in #TBSky but its an exciting time..
Some personal highlights (in no particular order):
1/10
Some personal highlights (in no particular order):
1/10