



Shino Kany
@shinokany.bsky.social
Cardiology and EP at UKE Hamburg, AI and Genetics at Broad Institute of MIT and Harvard.
Can a single ECG tell us who has coronary artery disease?
I’m excited to share the publication of our paper on using electrocardiogram-based artificial intelligence to predict prevalent coronary artery disease in @jaccjournals.bsky.social Advances.
I’m excited to share the publication of our paper on using electrocardiogram-based artificial intelligence to predict prevalent coronary artery disease in @jaccjournals.bsky.social Advances.

August 2, 2025 at 12:49 PM
Can a single ECG tell us who has coronary artery disease?
I’m excited to share the publication of our paper on using electrocardiogram-based artificial intelligence to predict prevalent coronary artery disease in @jaccjournals.bsky.social Advances.
I’m excited to share the publication of our paper on using electrocardiogram-based artificial intelligence to predict prevalent coronary artery disease in @jaccjournals.bsky.social Advances.
Im very honored to have been awarded with the Young Investigator Award "Arrhythmia" at the 91st annual meeting of the German Cardiac Society for our work on using clinical, genetic and AI risk for prediction of AF risk. Thanks for all co-authors and my mentors Shaan Khurshid and Patrick Ellinor.

April 27, 2025 at 2:08 PM
Im very honored to have been awarded with the Young Investigator Award "Arrhythmia" at the 91st annual meeting of the German Cardiac Society for our work on using clinical, genetic and AI risk for prediction of AF risk. Thanks for all co-authors and my mentors Shaan Khurshid and Patrick Ellinor.
Reposted by Shino Kany

Ever written an entire paper to fill out two empty cells in a table?
Along with @shinokany.bsky.social and colleagues, we did just that: proposing cutoffs for mild aortic stenosis using mean gradient, peak velocity, and aortic valve area (AVA). Free article:
authors.elsevier.com/a/1ks2B2d9GI...
Along with @shinokany.bsky.social and colleagues, we did just that: proposing cutoffs for mild aortic stenosis using mean gradient, peak velocity, and aortic valve area (AVA). Free article:
authors.elsevier.com/a/1ks2B2d9GI...

April 1, 2025 at 2:31 PM
Ever written an entire paper to fill out two empty cells in a table?
Along with @shinokany.bsky.social and colleagues, we did just that: proposing cutoffs for mild aortic stenosis using mean gradient, peak velocity, and aortic valve area (AVA). Free article:
authors.elsevier.com/a/1ks2B2d9GI...
Along with @shinokany.bsky.social and colleagues, we did just that: proposing cutoffs for mild aortic stenosis using mean gradient, peak velocity, and aortic valve area (AVA). Free article:
authors.elsevier.com/a/1ks2B2d9GI...
Happy to share our study “New Threshold for Defining Mild Aortic Stenosis Derived From Velocity-Encoded MRI in 60,000 Individuals” in which we identify a new threshold for Mild AS and the consequences of early aortic valve dysfunction. @jamespirruccello.com
authors.elsevier.com/a/1ks2B2d9GI...
authors.elsevier.com/a/1ks2B2d9GI...

April 1, 2025 at 3:31 AM
Happy to share our study “New Threshold for Defining Mild Aortic Stenosis Derived From Velocity-Encoded MRI in 60,000 Individuals” in which we identify a new threshold for Mild AS and the consequences of early aortic valve dysfunction. @jamespirruccello.com
authors.elsevier.com/a/1ks2B2d9GI...
authors.elsevier.com/a/1ks2B2d9GI...
I am excited to share our latest study published @jaccjournals.bsky.social Adv. We found that meeting guideline-recommended physical activity (PA) levels—whether as a “weekend warrior” or via regular activity—is linked to lower visceral and pericardial fat.
www.sciencedirect.com/science/arti...
www.sciencedirect.com/science/arti...
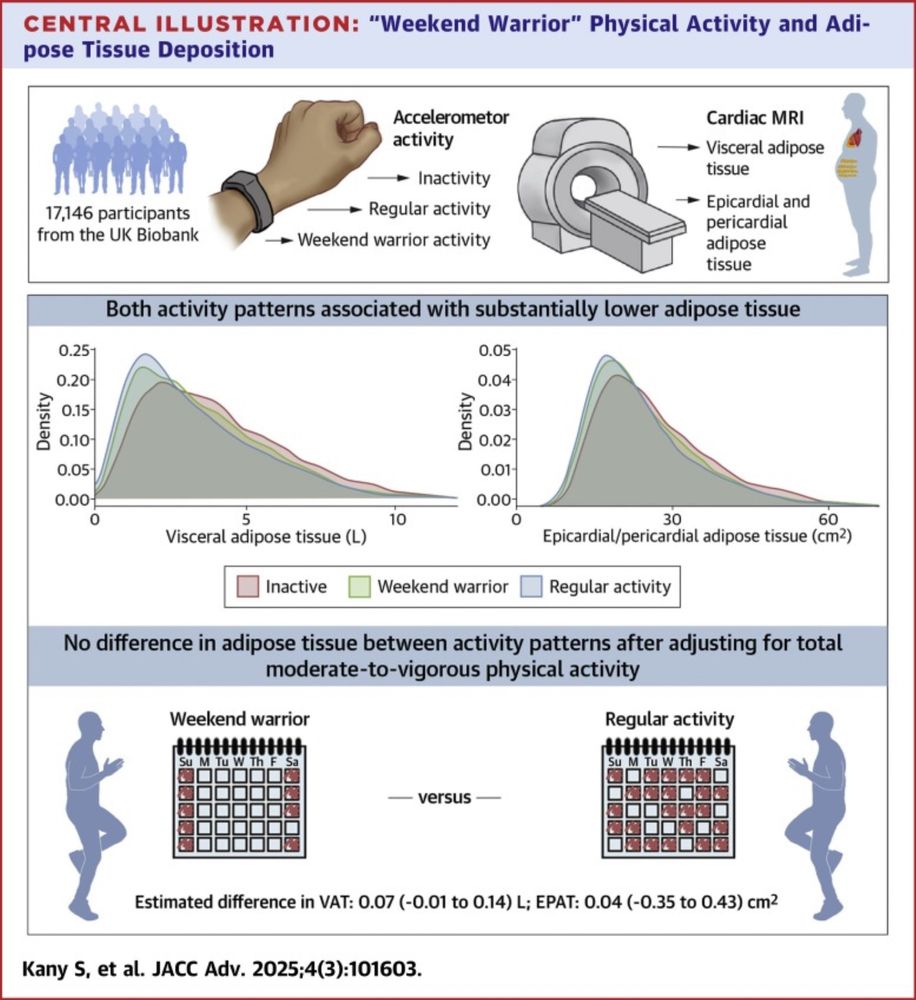
“Weekend Warrior” Physical Activity and Adipose Tissue Deposition
Attaining guideline-recommended levels of physical activity is associated with substantially lower risk of cardiometabolic diseases.Although physical …
www.sciencedirect.com
February 18, 2025 at 8:08 PM
I am excited to share our latest study published @jaccjournals.bsky.social Adv. We found that meeting guideline-recommended physical activity (PA) levels—whether as a “weekend warrior” or via regular activity—is linked to lower visceral and pericardial fat.
www.sciencedirect.com/science/arti...
www.sciencedirect.com/science/arti...