



Dilip Jayasimhan
@dilipj1.bsky.social
Respiratory physician and intensive care fellow 🇲🇾 🇳🇿
EOLIA had a 60-day mortality of 35% in the ECMO group. It's unlikely, I believe, that PP would reduce mortality by 15% in this group, let alone at the levels observed in PROSEVA, given that ECMO allows a safe reduction in driving pressure, one of the benefits of PP.

June 9, 2025 at 9:28 AM
EOLIA had a 60-day mortality of 35% in the ECMO group. It's unlikely, I believe, that PP would reduce mortality by 15% in this group, let alone at the levels observed in PROSEVA, given that ECMO allows a safe reduction in driving pressure, one of the benefits of PP.
Power calculations for PROSEVA estimated a 28d mortality of 60% in the control group and required enrolling 456 patients for 90% power to detect a 15% absolute reduction in mortality. The mortality in the control group was higher at 75%, with PP mortality of 38%. The true effect is likely smaller.

June 9, 2025 at 9:28 AM
Power calculations for PROSEVA estimated a 28d mortality of 60% in the control group and required enrolling 456 patients for 90% power to detect a 15% absolute reduction in mortality. The mortality in the control group was higher at 75%, with PP mortality of 38%. The true effect is likely smaller.
This trial showed no significant difference in mortality but ⬇️ incidence of ARDS and improved SOFA scores compared to placebo. There was no difference in the dichotomised cell-free Hb (CFH), but there was a suggestion that the higher the CFH, the higher the effect of PCM. (5/7)

December 2, 2024 at 11:05 AM
This trial showed no significant difference in mortality but ⬇️ incidence of ARDS and improved SOFA scores compared to placebo. There was no difference in the dichotomised cell-free Hb (CFH), but there was a suggestion that the higher the CFH, the higher the effect of PCM. (5/7)
1) That paracetamol hastens recovery in those destined to survive or prolongs death in those destined to die. OR
2) The effect of PCM/APAP is small and not captured well with a trial of this size, with possibly many patients not susceptible to the effect. (2/7)
2) The effect of PCM/APAP is small and not captured well with a trial of this size, with possibly many patients not susceptible to the effect. (2/7)

December 2, 2024 at 11:05 AM
1) That paracetamol hastens recovery in those destined to survive or prolongs death in those destined to die. OR
2) The effect of PCM/APAP is small and not captured well with a trial of this size, with possibly many patients not susceptible to the effect. (2/7)
2) The effect of PCM/APAP is small and not captured well with a trial of this size, with possibly many patients not susceptible to the effect. (2/7)
Tried to make sense of all the evidence before.
www.bjaed.org/article/S205...
www.bjaed.org/article/S205...

November 30, 2024 at 10:25 AM
Tried to make sense of all the evidence before.
www.bjaed.org/article/S205...
www.bjaed.org/article/S205...
Dead-space probably has an interaction with driving pressure. We've shown in this meta-analysis that it predicts mortality independent of compliance (especially when directly measured). What exactly that interaction is, however, remains unclear. #emimcc journals.lww.com/ccmjournal/a...

November 30, 2024 at 12:39 AM
Dead-space probably has an interaction with driving pressure. We've shown in this meta-analysis that it predicts mortality independent of compliance (especially when directly measured). What exactly that interaction is, however, remains unclear. #emimcc journals.lww.com/ccmjournal/a...
STAMINA showed only a 0.7 cmH20 difference in driving pressure between both arms. Compare this with ARMA, which (similar PEEP strategy in both arms) showed a Δ ~ 8 cmH20. Also note the baseline driving pressure was 13 cmH20, which isn’t terribly high (in reference to expected effect estimate below)

November 29, 2024 at 10:35 AM
STAMINA showed only a 0.7 cmH20 difference in driving pressure between both arms. Compare this with ARMA, which (similar PEEP strategy in both arms) showed a Δ ~ 8 cmH20. Also note the baseline driving pressure was 13 cmH20, which isn’t terribly high (in reference to expected effect estimate below)
Statistically, the driving pressure can be thought of as the interaction between tidal volume and respiratory system compliance. What was observed in the low tidal volume ventilation trials was the magnitude of the effect of low tidal volume on mortality was dependent on the compliance.

November 29, 2024 at 10:35 AM
Statistically, the driving pressure can be thought of as the interaction between tidal volume and respiratory system compliance. What was observed in the low tidal volume ventilation trials was the magnitude of the effect of low tidal volume on mortality was dependent on the compliance.
BLING-3 trial (and subsequent meta-analysis). I believe these studies will change practice in the years to come as we see the use of continuous infusions for beta-lactams improve outcomes among ICU patients. jamanetwork.com/journals/jam...

November 27, 2024 at 5:16 AM
BLING-3 trial (and subsequent meta-analysis). I believe these studies will change practice in the years to come as we see the use of continuous infusions for beta-lactams improve outcomes among ICU patients. jamanetwork.com/journals/jam...
Along the lines of ARDS, the EOLIA trial has truly established ECMO's role in management. It is what I would call the most positive negative trial published in critical care, which is why I believe its interpretation should take into account one’s priors as well as this Bayesian re-analysis.


November 27, 2024 at 5:16 AM
Along the lines of ARDS, the EOLIA trial has truly established ECMO's role in management. It is what I would call the most positive negative trial published in critical care, which is why I believe its interpretation should take into account one’s priors as well as this Bayesian re-analysis.
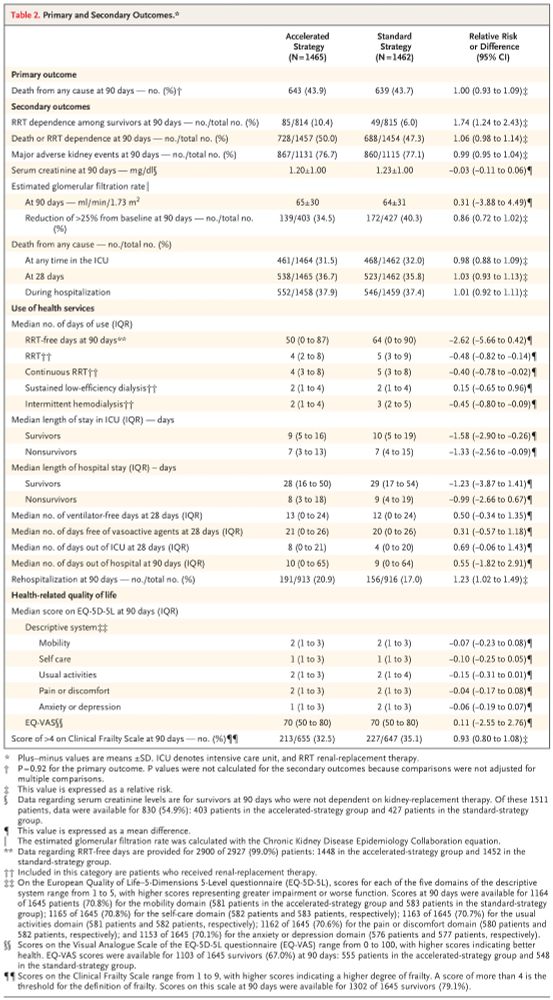
STARTT-AKI (along with AKIKI and IDEAL-ICU). The idea of renal supportive tx (early RRT to support kidney fx) was a growing concept. This trial exemplifies that in most cases, doing less is more. Although, waiting too long may have adverse consequences (AKIKI-2) maing me consider urea as well
November 27, 2024 at 5:16 AM
STARTT-AKI (along with AKIKI and IDEAL-ICU). The idea of renal supportive tx (early RRT to support kidney fx) was a growing concept. This trial exemplifies that in most cases, doing less is more. Although, waiting too long may have adverse consequences (AKIKI-2) maing me consider urea as well
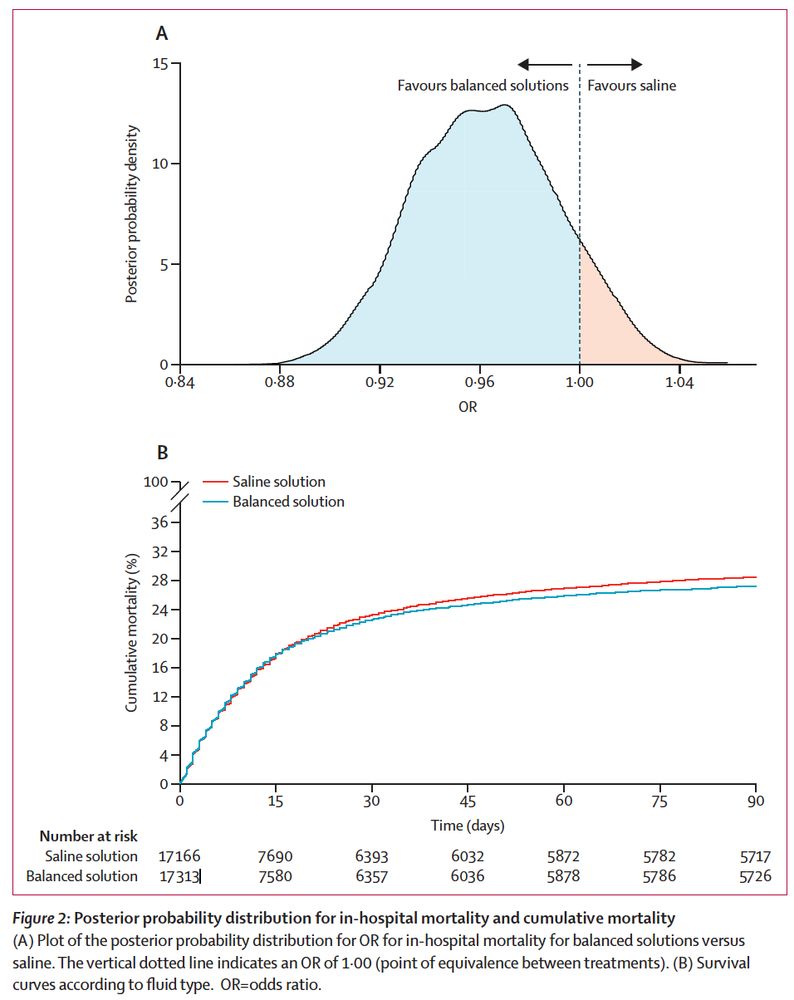
BEST-LIVING with its associated trials (SPLIT, SMART, SALT-ED, SCOPE-DKA, and PLUS). Many arguments are made that fluid tx should be based on physiological parameters such as Na and Cl levels. This IPDMA shows no point estimate favouring saline favouring these parameters (apart from TBI).

November 27, 2024 at 5:16 AM
BEST-LIVING with its associated trials (SPLIT, SMART, SALT-ED, SCOPE-DKA, and PLUS). Many arguments are made that fluid tx should be based on physiological parameters such as Na and Cl levels. This IPDMA shows no point estimate favouring saline favouring these parameters (apart from TBI).
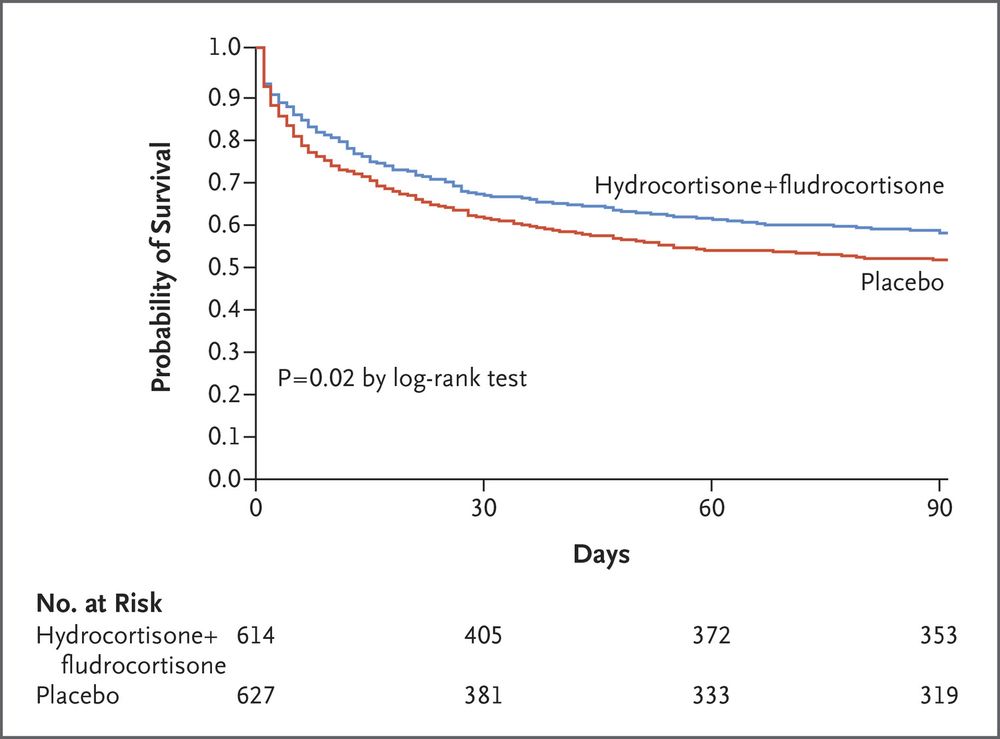
ADRENAL and APPROCHS. I remember strong scepticism about the utility of steroids in septic shock. I believe the scepticism has at least reduced. A special mention to the Dequin study showing a favourable effect in severe pneumonia, which I believe to be the next frontier for corticosteroid use.

November 27, 2024 at 5:16 AM
ADRENAL and APPROCHS. I remember strong scepticism about the utility of steroids in septic shock. I believe the scepticism has at least reduced. A special mention to the Dequin study showing a favourable effect in severe pneumonia, which I believe to be the next frontier for corticosteroid use.
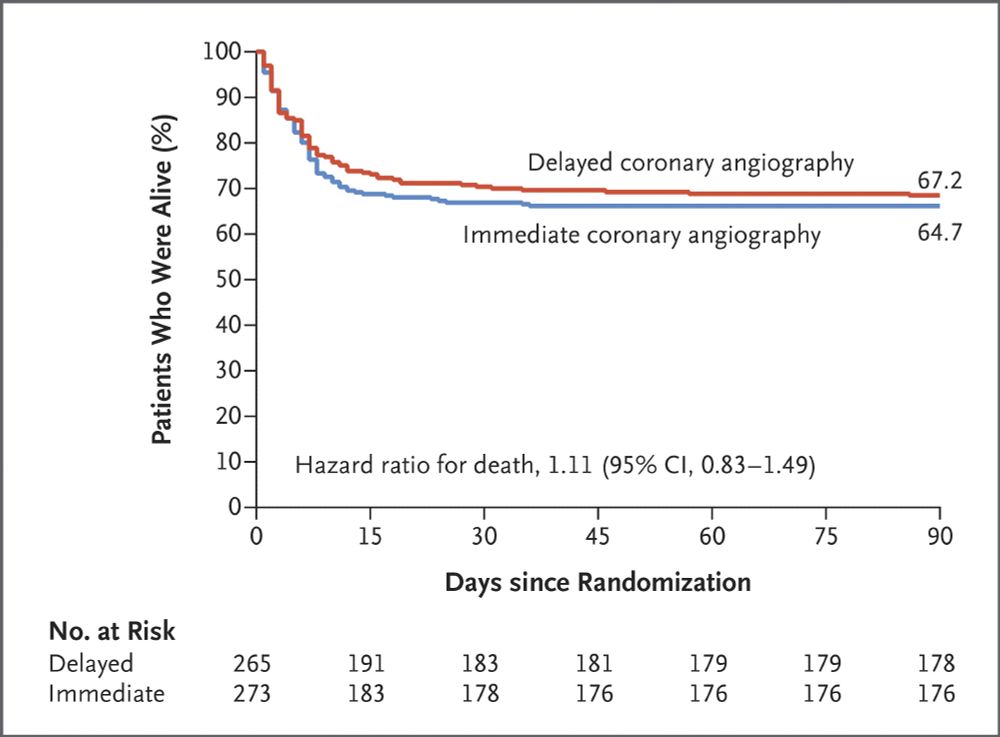
TOMAHAWK and COACT. In a hospital I had worked in, the disposition (cardiac vs general ICU) of a patient following an OHCA was dependent on the coronary angiogram they received on arrival. These trials have challenged long-held dogma.

November 27, 2024 at 5:16 AM
TOMAHAWK and COACT. In a hospital I had worked in, the disposition (cardiac vs general ICU) of a patient following an OHCA was dependent on the coronary angiogram they received on arrival. These trials have challenged long-held dogma.
When many of these interventions are tested in larger multicentre trials, the estimate of effect is not commonly replicated. ccforum.biomedcentral.com/articles/10.... #emimcc

November 23, 2024 at 12:25 AM
When many of these interventions are tested in larger multicentre trials, the estimate of effect is not commonly replicated. ccforum.biomedcentral.com/articles/10.... #emimcc
Single centre trials tend to have a higher rate of falsely positive results for many reasons. Statistically, this paper illustrates this phenomenon quite well www.bjanaesthesia.org.uk/article/S000... #emimcc

November 23, 2024 at 12:23 AM
Single centre trials tend to have a higher rate of falsely positive results for many reasons. Statistically, this paper illustrates this phenomenon quite well www.bjanaesthesia.org.uk/article/S000... #emimcc
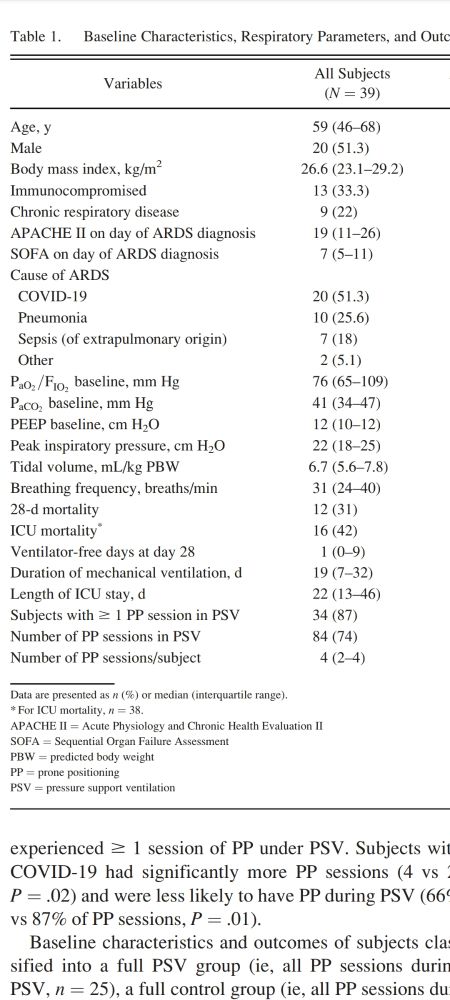
Half the patients had a PaO2/FiO2 of 76 or less and 3 quarters < 109. Which feels like the kind of patients I would prone. Not suggesting this be implemented but the dogma of deep sedation and paralysis should be explored with appropriate trials. Feasibility is usually an impeding factor to this
November 22, 2024 at 3:07 AM
Half the patients had a PaO2/FiO2 of 76 or less and 3 quarters < 109. Which feels like the kind of patients I would prone. Not suggesting this be implemented but the dogma of deep sedation and paralysis should be explored with appropriate trials. Feasibility is usually an impeding factor to this