



Dilip Jayasimhan
@dilipj1.bsky.social
Respiratory physician and intensive care fellow 🇲🇾 🇳🇿
On the note of VAP, we've written a review article. More specifically, focusing on the evidence behind strategies to prevent and manage VAP. This link gives 50 days of free access. Hope you all find it useful. #emimcc
authors.elsevier.com/a/1lbEr7K3e2...
authors.elsevier.com/a/1lbEr7K3e2...
August 13, 2025 at 10:46 AM
On the note of VAP, we've written a review article. More specifically, focusing on the evidence behind strategies to prevent and manage VAP. This link gives 50 days of free access. Hope you all find it useful. #emimcc
authors.elsevier.com/a/1lbEr7K3e2...
authors.elsevier.com/a/1lbEr7K3e2...
Reposted by Dilip Jayasimhan

Insulin gtt + usual management. Oral triglyceride meds going forward.
July 10, 2025 at 8:34 PM
Insulin gtt + usual management. Oral triglyceride meds going forward.
Reposted by Dilip Jayasimhan

Nice thread. Well summarised. Thank you. Imho- prone ventilation helps homogenise distribution of mechanical power. If on VV and on “rest” ventilation (whatever that is since no consensus on what rest is whilst ELSo guidelines allude to) then the benefit from proning is v minimal
June 9, 2025 at 2:01 PM
Nice thread. Well summarised. Thank you. Imho- prone ventilation helps homogenise distribution of mechanical power. If on VV and on “rest” ventilation (whatever that is since no consensus on what rest is whilst ELSo guidelines allude to) then the benefit from proning is v minimal
I think, given that it took many trials with different sample sizes and durations of proning for us to realise its effectiveness in ARDS without ECMO, it would be even harder to prove in patients on ECMO for several reasons. COI: I love to prone 🧵 #emimcc
interesting editorial on proning during VV-ECMO
the sequence of [#1] VV-ECMO without a prone trial, and then [#2] proning while on VV-ECMO seems 🍑 backwards
and proning while on VV-ECMO doesn't seem awesome (c/w the largest RCT)
(but there may be situations where this makes sense 🤷♂️) #EMIMCC
the sequence of [#1] VV-ECMO without a prone trial, and then [#2] proning while on VV-ECMO seems 🍑 backwards
and proning while on VV-ECMO doesn't seem awesome (c/w the largest RCT)
(but there may be situations where this makes sense 🤷♂️) #EMIMCC



June 9, 2025 at 9:28 AM
I think, given that it took many trials with different sample sizes and durations of proning for us to realise its effectiveness in ARDS without ECMO, it would be even harder to prove in patients on ECMO for several reasons. COI: I love to prone 🧵 #emimcc
I don't have strong opinions about APRV, but I think the utility and effectiveness of certain strategies depend heavily on the system within which they work. #EMIMCC
Should APRV remain part of the recommendations in severe ARDS, and should a trial be considered before VV ECMO referral?
Discuss. #emimcc
@pulmcrit.bsky.social @icmtim.bsky.social
Open DOI: our ECMO centre doesn’t recommend APRV…
Discuss. #emimcc
@pulmcrit.bsky.social @icmtim.bsky.social
Open DOI: our ECMO centre doesn’t recommend APRV…

Having spoken to them - it was recognised that cARDS didn't respond to PEEP as non-cARDS. V/Q mismatch was increasingly recognised. One size does not fit all. As with high PEEP, APRV will help some patients, not others.
ARPV regularly recommended as a trial by centres as I say.
ARPV regularly recommended as a trial by centres as I say.
June 6, 2025 at 1:28 AM
I don't have strong opinions about APRV, but I think the utility and effectiveness of certain strategies depend heavily on the system within which they work. #EMIMCC
A well written argument cautioning against misinterpreting evidence from clinical trials on angiotensin II. Currently, A-II is not available outside a clinical trial where I work. However, there are efforts to evaluate A-II in other populations (not sepsis). pmc.ncbi.nlm.nih.gov/articles/PMC...
June 4, 2025 at 10:15 AM
A well written argument cautioning against misinterpreting evidence from clinical trials on angiotensin II. Currently, A-II is not available outside a clinical trial where I work. However, there are efforts to evaluate A-II in other populations (not sepsis). pmc.ncbi.nlm.nih.gov/articles/PMC...
Reposted by Dilip Jayasimhan

I rather think it’s action bias, easier to do something than to wait and see. People overestimate the risk of deterioration and underestimate bleeding risk.
May 26, 2025 at 5:19 AM
I rather think it’s action bias, easier to do something than to wait and see. People overestimate the risk of deterioration and underestimate bleeding risk.
Reposted by Dilip Jayasimhan

interesting thread with some great points here 👇
IMHO the key is having an institutional pathway about classification & management that everybody agrees on
for patients in whom the treatment pathway is clear, there is no need to involve everybody (eg, if clearly not an IR candidate, why call IR?)
IMHO the key is having an institutional pathway about classification & management that everybody agrees on
for patients in whom the treatment pathway is clear, there is no need to involve everybody (eg, if clearly not an IR candidate, why call IR?)
My unpopular opinion is that I'm skeptical about the effectiveness of PERT. 🧵 #EMIMCC
it's largely impossible to handle a PERT (PE response team) call *without* a CT angiogram
even if the RV looks horrible on POCUS, this doesn't differentiate between acute PE vs chronic pulm HTN (which is common in older, multimorbid pts)
unless pt is in extremis, start with a CT angio. #EMIMCC
even if the RV looks horrible on POCUS, this doesn't differentiate between acute PE vs chronic pulm HTN (which is common in older, multimorbid pts)
unless pt is in extremis, start with a CT angio. #EMIMCC
May 25, 2025 at 12:08 PM
interesting thread with some great points here 👇
IMHO the key is having an institutional pathway about classification & management that everybody agrees on
for patients in whom the treatment pathway is clear, there is no need to involve everybody (eg, if clearly not an IR candidate, why call IR?)
IMHO the key is having an institutional pathway about classification & management that everybody agrees on
for patients in whom the treatment pathway is clear, there is no need to involve everybody (eg, if clearly not an IR candidate, why call IR?)
Reposted by Dilip Jayasimhan

Similar arguments could be made perhaps for “shock” teams
🤔
🤔
May 25, 2025 at 12:17 PM
Similar arguments could be made perhaps for “shock” teams
🤔
🤔
Reposted by Dilip Jayasimhan
Could not agree more! The problem with pulmonary embolism is the lack of clear ownership (at least in my part of the world). #emimcc #cardiosky
Cardiologists don't congregate when a STEMI comes through the door, nor do neurologists when a stroke is admitted. Partly because there is ownership by one specialty, and because there is high quality evidence to guide management. Evidence rather than eminence based medicine.
May 25, 2025 at 12:48 PM
Could not agree more! The problem with pulmonary embolism is the lack of clear ownership (at least in my part of the world). #emimcc #cardiosky
My unpopular opinion is that I'm skeptical about the effectiveness of PERT. 🧵 #EMIMCC
it's largely impossible to handle a PERT (PE response team) call *without* a CT angiogram
even if the RV looks horrible on POCUS, this doesn't differentiate between acute PE vs chronic pulm HTN (which is common in older, multimorbid pts)
unless pt is in extremis, start with a CT angio. #EMIMCC
even if the RV looks horrible on POCUS, this doesn't differentiate between acute PE vs chronic pulm HTN (which is common in older, multimorbid pts)
unless pt is in extremis, start with a CT angio. #EMIMCC

a heart with a picture of a girl and the words " pert my beloved " on it
ALT: a heart with a picture of a girl and the words " pert my beloved " on it
media.tenor.com
May 25, 2025 at 10:18 AM
My unpopular opinion is that I'm skeptical about the effectiveness of PERT. 🧵 #EMIMCC
An interesting issue of ICU Management & Practice. From Sepsis to ARDS. #EMIMCC healthmanagement.org/c/icu/issue/...

Volume 25 - Issue 2, 2025
Change content default value...
healthmanagement.org
May 25, 2025 at 3:43 AM
An interesting issue of ICU Management & Practice. From Sepsis to ARDS. #EMIMCC healthmanagement.org/c/icu/issue/...
The final interim analysis for the #MegaROX trial, including the first 32000 patients enrolled, is happening soon.

February 26, 2025 at 6:22 AM
I disagree with the conclusion reached here. I have previously written a thread on this, which I have linked below. #emimcc

Clinical Conundrum: Should We Always Treat Fever in Sepsis?: bit.ly/3BwUEbq
TL;DR: No. No incr mortality/morbidity + possible protective effects
#MedSky #EMIMCC
TL;DR: No. No incr mortality/morbidity + possible protective effects
#MedSky #EMIMCC

December 18, 2024 at 10:51 AM
I disagree with the conclusion reached here. I have previously written a thread on this, which I have linked below. #emimcc
Reposted by Dilip Jayasimhan
What I love about echocardiography in critical care is how you can see physiology unfolding before your eyes. This is a case that has stayed with me and shaped how I think about treating acute LVOT obstruction #cccsky #echofirst #pocus #emimcc
A case both for not forgetting basic physical examination including auscultation and for echo in shock. Shared with patients consent. 🧵 #foamcc #foamed
December 4, 2024 at 10:34 PM
What I love about echocardiography in critical care is how you can see physiology unfolding before your eyes. This is a case that has stayed with me and shaped how I think about treating acute LVOT obstruction #cccsky #echofirst #pocus #emimcc
Reposted by Dilip Jayasimhan

Are you interested in #Sustainability in #Anesthesiology and how reusing TIVA lines could help reduce greenhouse gas emissions? Per Werner Moller, originally an expert in #AppliedPhysiology and #VenousReturn, discusses their environmental paper on the #EJA podcast.
open.spotify.com/episode/2RCa...
open.spotify.com/episode/2RCa...
December 3, 2024 at 9:36 PM
Are you interested in #Sustainability in #Anesthesiology and how reusing TIVA lines could help reduce greenhouse gas emissions? Per Werner Moller, originally an expert in #AppliedPhysiology and #VenousReturn, discusses their environmental paper on the #EJA podcast.
open.spotify.com/episode/2RCa...
open.spotify.com/episode/2RCa...
Had a similar case of someone with disproportionate hypoxaemia in the context of an intermediate risk PE. Pt was also hypertensive. #emimcc #pulmsky #medsky
An older but very functional patient presented from another facility to the neuro ICU with a brain abscess after a dental procedure.
The abscess was being treated conservatively and was improving.
Pulm was consulted for hypoxia.
#emimcc
The abscess was being treated conservatively and was improving.
Pulm was consulted for hypoxia.
#emimcc
December 3, 2024 at 1:24 AM
This trial always fascinated me. It's extremely informative and with other evidence (ASTER), makes you wonder about the benefit of PCM/APAP in sepsis. Primary outcome was neutral, but PCM/APAP ⬇️ ICU LOS in survivors and ⬆️ ICU LOS in non-survivors. This can mean one of 2 things (1/7)🧵 #emimcc #medsky

Might be something to this for peds, but for adult sepsis, we have pretty good data:
www.nejm.org/doi/full/10....
www.nejm.org/doi/full/10....

Acetaminophen for Fever in Critically Ill Patients with Suspected Infection | NEJM
Acetaminophen is a common therapy for fever in patients in the intensive care unit
(ICU) who have probable infection, but its effects are unknown. We randomly assigned
700 ICU patients with fever (...
www.nejm.org
December 2, 2024 at 11:05 AM
This trial always fascinated me. It's extremely informative and with other evidence (ASTER), makes you wonder about the benefit of PCM/APAP in sepsis. Primary outcome was neutral, but PCM/APAP ⬇️ ICU LOS in survivors and ⬆️ ICU LOS in non-survivors. This can mean one of 2 things (1/7)🧵 #emimcc #medsky
Reposted by Dilip Jayasimhan
It's unethical not to adjust for a priori important baseline characteristics predictive of the outcome!
#stats #medsky #metascience
#stats #medsky #metascience
When interpreting this trial, it is also important to consider the pre-specified adjusted analysis [OR 0.89 (95%CI 0.79 to 0.99)] as adjustment improves statistical efficiency. This article explains the benefits of adjustment quite well. #emimcc jamanetwork.com/journals/jam...
December 1, 2024 at 11:01 PM
It's unethical not to adjust for a priori important baseline characteristics predictive of the outcome!
#stats #medsky #metascience
#stats #medsky #metascience
When interpreting this trial, it is also important to consider the pre-specified adjusted analysis [OR 0.89 (95%CI 0.79 to 0.99)] as adjustment improves statistical efficiency. This article explains the benefits of adjustment quite well. #emimcc jamanetwork.com/journals/jam...
December 1, 2024 at 4:36 AM
When interpreting this trial, it is also important to consider the pre-specified adjusted analysis [OR 0.89 (95%CI 0.79 to 0.99)] as adjustment improves statistical efficiency. This article explains the benefits of adjustment quite well. #emimcc jamanetwork.com/journals/jam...
Reposted by Dilip Jayasimhan
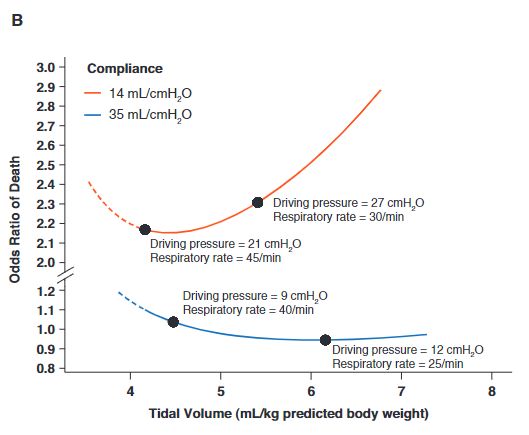
I agree, in a Vt range of 6-8 ml, the main component is dP. However, if you target low/very low dP (12-15) in a patient with poor compliance (very low tidal ventilation) and the increase in respiratory rate becomes relevant, I think. The figure is from the excellent paper you referenced (thanks).
November 29, 2024 at 12:52 PM
I agree, in a Vt range of 6-8 ml, the main component is dP. However, if you target low/very low dP (12-15) in a patient with poor compliance (very low tidal ventilation) and the increase in respiratory rate becomes relevant, I think. The figure is from the excellent paper you referenced (thanks).
This trial evaluating a driving pressure limiting strategy to standard care in patients with pneumonia and ARDS showed no difference in ventilator-free days. However, I have a few thoughts on it. 🧵

'In patients with moderate to severe ARDS secondary to community-acquired pneumonia, a driving pressure-limiting strategy did not increase the number of ventilator-free days compared with a standard low PEEP strategy' #critcaresky #emimcc
pubmed.ncbi.nlm.nih.gov/39592365/
pubmed.ncbi.nlm.nih.gov/39592365/

Effect of a driving pressure-limiting strategy for patients with acute respiratory distress syndrome secondary to community-acquired pneumonia: the STAMINA randomised clinical trial - PubMed
NCT04972318.
pubmed.ncbi.nlm.nih.gov
November 29, 2024 at 10:35 AM
This trial evaluating a driving pressure limiting strategy to standard care in patients with pneumonia and ARDS showed no difference in ventilator-free days. However, I have a few thoughts on it. 🧵
Reposted by Dilip Jayasimhan

A treasure trove of important trials for ICM trainees to sink their teeth into
Nice work @dilipj1.bsky.social 🙌
Nice work @dilipj1.bsky.social 🙌
A thread 🧵 on trials I think have changed or will change ICU practice (at least my own). #emimcc

At the back of Revision Notes In Intensive Care Medicine there is a list of 59 key papers relating to intensive care medicine published between 1998 and 2015 (the book was published in 2016).
I'd like to keep my revision up to date. Are there any equivalent lists of key papers from 2016 to now?
I'd like to keep my revision up to date. Are there any equivalent lists of key papers from 2016 to now?
November 28, 2024 at 8:05 PM
A treasure trove of important trials for ICM trainees to sink their teeth into
Nice work @dilipj1.bsky.social 🙌
Nice work @dilipj1.bsky.social 🙌
Reposted by Dilip Jayasimhan

We are gearing up to offer our online course on Reimagining Global Health in summer 2025
For now, you can access last year's slides & readings here
www.teachepi.org/courses/reim...
For now, you can access last year's slides & readings here
www.teachepi.org/courses/reim...

November 27, 2024 at 3:03 PM
We are gearing up to offer our online course on Reimagining Global Health in summer 2025
For now, you can access last year's slides & readings here
www.teachepi.org/courses/reim...
For now, you can access last year's slides & readings here
www.teachepi.org/courses/reim...