




Tim Leeuwenburg
@kangaroobeach.bsky.social
#FOAMed #justaGP
Senior specialist at Central Australian Retrieval Service, Chair of SandpiperAustralia.org
Plus occasional work in rural anaesthesia, EM, VAD etc
@kangaroobeach - rural doc living on Kangaroo Island, SA
Senior specialist at Central Australian Retrieval Service, Chair of SandpiperAustralia.org
Plus occasional work in rural anaesthesia, EM, VAD etc
@kangaroobeach - rural doc living on Kangaroo Island, SA
COWs at night
I am a dinosaur
Perpetually perplexed by computers-on-wheels clogging up corridors and clinical spaces
I am a dinosaur
Perpetually perplexed by computers-on-wheels clogging up corridors and clinical spaces

September 25, 2025 at 9:57 PM
COWs at night
I am a dinosaur
Perpetually perplexed by computers-on-wheels clogging up corridors and clinical spaces
I am a dinosaur
Perpetually perplexed by computers-on-wheels clogging up corridors and clinical spaces
Intense prehospital emergency care (PHEC) course in regional Victoria, Aus
Helping rural docs translate their existing skills to prehospital scene, to support local ambulance for pts with time critical needs before retrieval arrive #traumagap
Immersive scenarios
Trauma
Burns
End of life
Etc etc
Helping rural docs translate their existing skills to prehospital scene, to support local ambulance for pts with time critical needs before retrieval arrive #traumagap
Immersive scenarios
Trauma
Burns
End of life
Etc etc




August 21, 2025 at 12:18 PM
Intense prehospital emergency care (PHEC) course in regional Victoria, Aus
Helping rural docs translate their existing skills to prehospital scene, to support local ambulance for pts with time critical needs before retrieval arrive #traumagap
Immersive scenarios
Trauma
Burns
End of life
Etc etc
Helping rural docs translate their existing skills to prehospital scene, to support local ambulance for pts with time critical needs before retrieval arrive #traumagap
Immersive scenarios
Trauma
Burns
End of life
Etc etc
Another PHEC (prehospital emergency care) course complete on Gold Coast today - 24 rural
Docs completing scenarios to help translate their existing skillset to prehospital, helping close #traumagap in rural
Oz needs rural responder networks to help improve outcomes where resources are limited
Docs completing scenarios to help translate their existing skillset to prehospital, helping close #traumagap in rural
Oz needs rural responder networks to help improve outcomes where resources are limited



June 26, 2025 at 8:29 AM
Another PHEC (prehospital emergency care) course complete on Gold Coast today - 24 rural
Docs completing scenarios to help translate their existing skillset to prehospital, helping close #traumagap in rural
Oz needs rural responder networks to help improve outcomes where resources are limited
Docs completing scenarios to help translate their existing skillset to prehospital, helping close #traumagap in rural
Oz needs rural responder networks to help improve outcomes where resources are limited
Wow
UK British Medical
association calls for new regulator given how compromised GMC is
activism.bma.org.uk/page/172664/...
UK British Medical
association calls for new regulator given how compromised GMC is
activism.bma.org.uk/page/172664/...

June 23, 2025 at 11:21 AM
Wow
UK British Medical
association calls for new regulator given how compromised GMC is
activism.bma.org.uk/page/172664/...
UK British Medical
association calls for new regulator given how compromised GMC is
activism.bma.org.uk/page/172664/...
Reposted by Tim Leeuwenburg
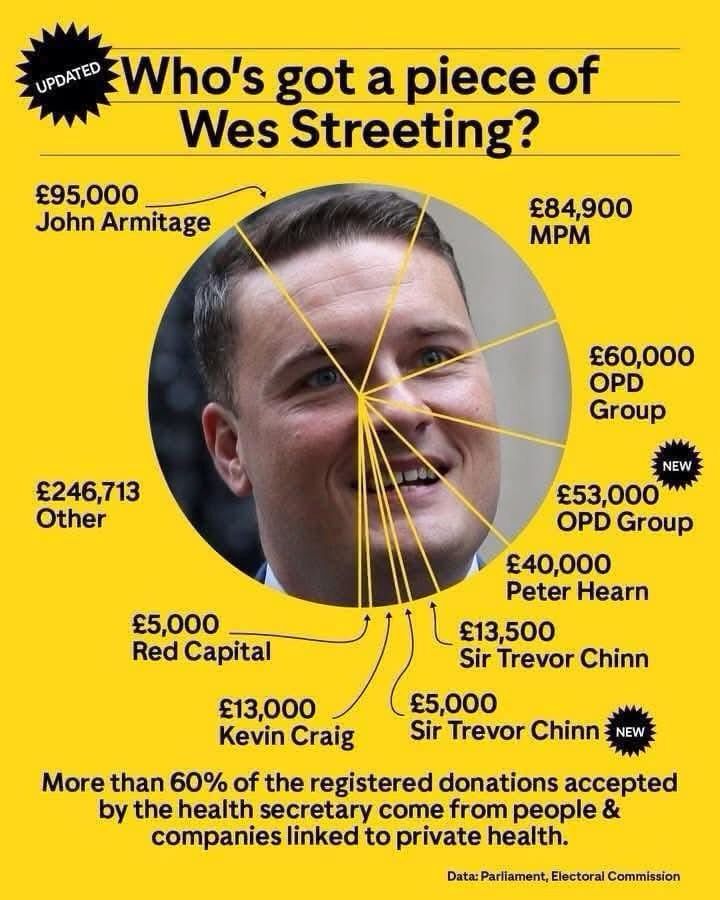
As a GP, I am not allowed to receive a pen or post-it note pad from a pharmaceutical company rep
The Government banned them in case I was influenced to prescribe a certain medication
This should also be banned @rthonwesstreeting.bsky.social unless you have a way to justify this?
The Government banned them in case I was influenced to prescribe a certain medication
This should also be banned @rthonwesstreeting.bsky.social unless you have a way to justify this?
May 5, 2025 at 5:04 PM
As a GP, I am not allowed to receive a pen or post-it note pad from a pharmaceutical company rep
The Government banned them in case I was influenced to prescribe a certain medication
This should also be banned @rthonwesstreeting.bsky.social unless you have a way to justify this?
The Government banned them in case I was influenced to prescribe a certain medication
This should also be banned @rthonwesstreeting.bsky.social unless you have a way to justify this?
Reposted by Tim Leeuwenburg
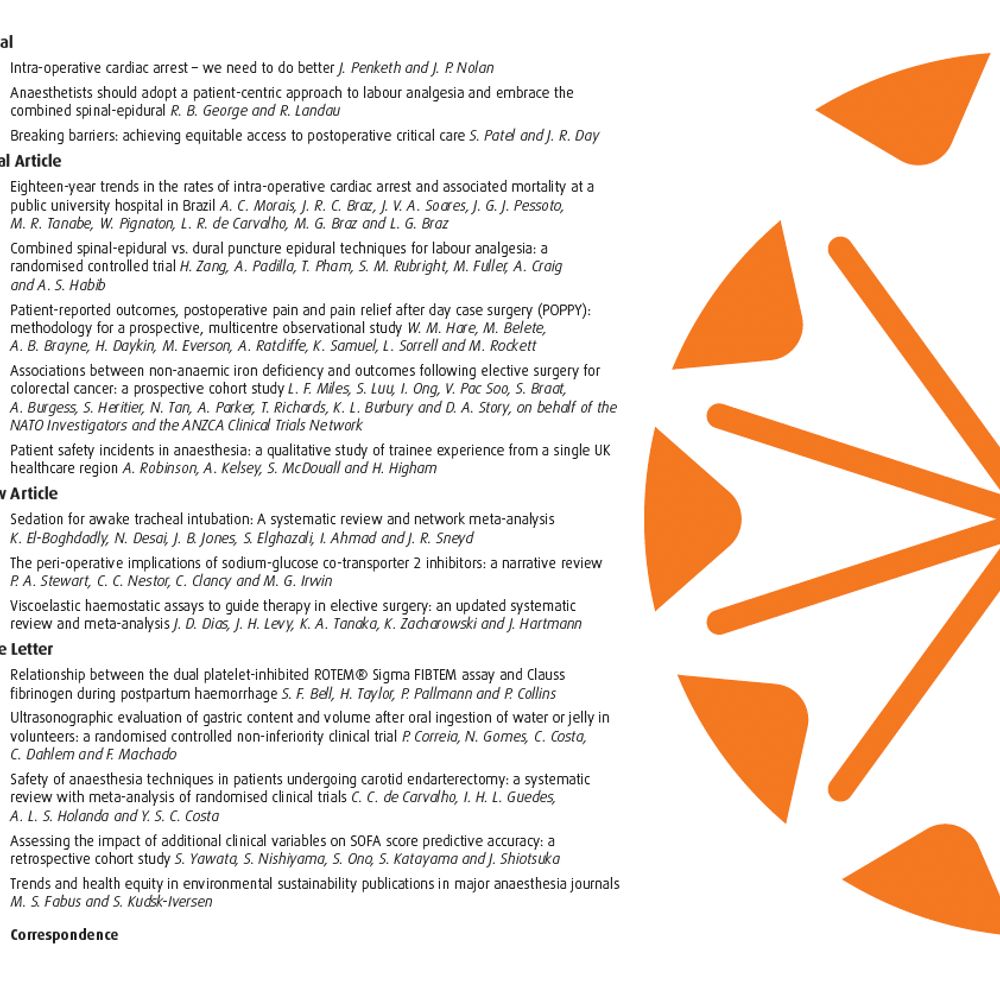
I think it is evident that we have already brought the conversation to BlueSky!
In an environment plagued by scientific misinformation, do medical organisations/journals have a moral imperative to remain, to provide a source of truth & reason?
Or should they just.. leave?
Let's discuss.
#AnSky
In an environment plagued by scientific misinformation, do medical organisations/journals have a moral imperative to remain, to provide a source of truth & reason?
Or should they just.. leave?
Let's discuss.
#AnSky
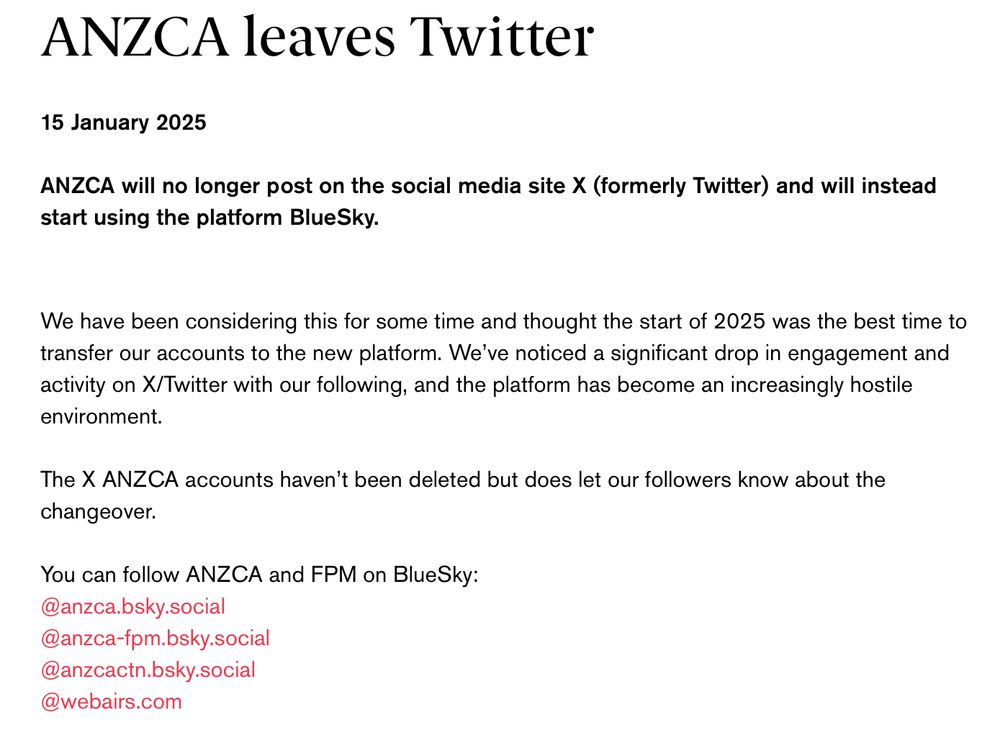
Huge respect to @anzca.bsky.social for leaving Twitter behind. Time for other health related organisations to do the same.
You have the power to bring the conversation to BlueSky.
@safeairwaysociety.org @rcoanews.bsky.social @anaesjournal.bsky.social
@bjajournals.bsky.social
#ASM25CNS
You have the power to bring the conversation to BlueSky.
@safeairwaysociety.org @rcoanews.bsky.social @anaesjournal.bsky.social
@bjajournals.bsky.social
#ASM25CNS

May 5, 2025 at 8:24 AM
I think it is evident that we have already brought the conversation to BlueSky!
In an environment plagued by scientific misinformation, do medical organisations/journals have a moral imperative to remain, to provide a source of truth & reason?
Or should they just.. leave?
Let's discuss.
#AnSky
In an environment plagued by scientific misinformation, do medical organisations/journals have a moral imperative to remain, to provide a source of truth & reason?
Or should they just.. leave?
Let's discuss.
#AnSky
Evening Brisbane!
Hectic circuit from Cairns-Melbourne-Brisbane for @etmcourse.bsky.social
Next three days will be challenge attendees with scenarios of increasing complexity…which will become easier due to training in generic resus room skills
- role allocation
- closed loop
- next 3 steps
Hectic circuit from Cairns-Melbourne-Brisbane for @etmcourse.bsky.social
Next three days will be challenge attendees with scenarios of increasing complexity…which will become easier due to training in generic resus room skills
- role allocation
- closed loop
- next 3 steps

May 6, 2025 at 8:18 AM
Evening Brisbane!
Hectic circuit from Cairns-Melbourne-Brisbane for @etmcourse.bsky.social
Next three days will be challenge attendees with scenarios of increasing complexity…which will become easier due to training in generic resus room skills
- role allocation
- closed loop
- next 3 steps
Hectic circuit from Cairns-Melbourne-Brisbane for @etmcourse.bsky.social
Next three days will be challenge attendees with scenarios of increasing complexity…which will become easier due to training in generic resus room skills
- role allocation
- closed loop
- next 3 steps
Reposted by Tim Leeuwenburg

In the #impostersyndrome we discount what we know and inflate what we think other people know. You know more than you think. Others know less than you think. You're not an imposter. #impostersyndrome #phdchat #ECRchat #PhdForum
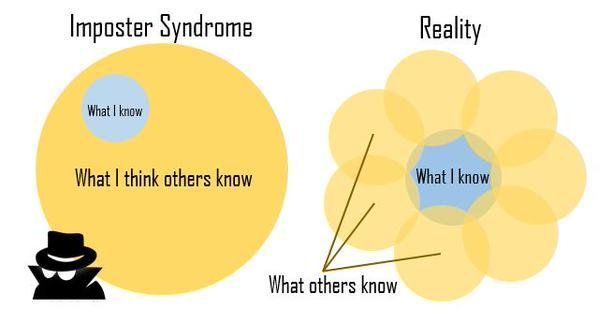
May 5, 2025 at 9:02 AM
In the #impostersyndrome we discount what we know and inflate what we think other people know. You know more than you think. Others know less than you think. You're not an imposter. #impostersyndrome #phdchat #ECRchat #PhdForum
So much this
Thanks @drglauco.bsky.social
Thoughts on American healthcare, insurance and accessibility….
Thanks @drglauco.bsky.social
Thoughts on American healthcare, insurance and accessibility….

May 5, 2025 at 4:33 AM
So much this
Thanks @drglauco.bsky.social
Thoughts on American healthcare, insurance and accessibility….
Thanks @drglauco.bsky.social
Thoughts on American healthcare, insurance and accessibility….
Reposted by Tim Leeuwenburg

This paper on BIS in @bjajournals.bsky.social (study done right here in Cairns) is one of my all time favourites.
Administration of NMBA alone drops BIS to 44 in completely awake subjects!
#ASM25CNS
academic.oup.com/bja/article/...
Administration of NMBA alone drops BIS to 44 in completely awake subjects!
#ASM25CNS
academic.oup.com/bja/article/...

May 4, 2025 at 10:58 PM
This paper on BIS in @bjajournals.bsky.social (study done right here in Cairns) is one of my all time favourites.
Administration of NMBA alone drops BIS to 44 in completely awake subjects!
#ASM25CNS
academic.oup.com/bja/article/...
Administration of NMBA alone drops BIS to 44 in completely awake subjects!
#ASM25CNS
academic.oup.com/bja/article/...
Reposted by Tim Leeuwenburg
Huge respect to @anzca.bsky.social for leaving Twitter behind. Time for other health related organisations to do the same.
You have the power to bring the conversation to BlueSky.
@safeairwaysociety.org @rcoanews.bsky.social @anaesjournal.bsky.social
@bjajournals.bsky.social
#ASM25CNS
You have the power to bring the conversation to BlueSky.
@safeairwaysociety.org @rcoanews.bsky.social @anaesjournal.bsky.social
@bjajournals.bsky.social
#ASM25CNS
May 5, 2025 at 12:50 AM
Huge respect to @anzca.bsky.social for leaving Twitter behind. Time for other health related organisations to do the same.
You have the power to bring the conversation to BlueSky.
@safeairwaysociety.org @rcoanews.bsky.social @anaesjournal.bsky.social
@bjajournals.bsky.social
#ASM25CNS
You have the power to bring the conversation to BlueSky.
@safeairwaysociety.org @rcoanews.bsky.social @anaesjournal.bsky.social
@bjajournals.bsky.social
#ASM25CNS
Cairns
Just completed theee days as director for an @etmcourse.bsky.social in this fabulous location
ANZCA ASM kicks off soon…
Just completed theee days as director for an @etmcourse.bsky.social in this fabulous location
ANZCA ASM kicks off soon…

April 30, 2025 at 7:50 AM
Cairns
Just completed theee days as director for an @etmcourse.bsky.social in this fabulous location
ANZCA ASM kicks off soon…
Just completed theee days as director for an @etmcourse.bsky.social in this fabulous location
ANZCA ASM kicks off soon…
Reposted by Tim Leeuwenburg

Inspired by posters going up in anaesthetic rooms at @ekhuft.bsky.social, I thought I'd share this again.
Error with TIVA is potentially more common, because multiple errors are not yet prevented by the equipment.
You can check your working with #PERUSEbeforeYouInfuse .
youtu.be/HGtBMHXUVyA?...
Error with TIVA is potentially more common, because multiple errors are not yet prevented by the equipment.
You can check your working with #PERUSEbeforeYouInfuse .
youtu.be/HGtBMHXUVyA?...

April 20, 2025 at 7:52 AM
Inspired by posters going up in anaesthetic rooms at @ekhuft.bsky.social, I thought I'd share this again.
Error with TIVA is potentially more common, because multiple errors are not yet prevented by the equipment.
You can check your working with #PERUSEbeforeYouInfuse .
youtu.be/HGtBMHXUVyA?...
Error with TIVA is potentially more common, because multiple errors are not yet prevented by the equipment.
You can check your working with #PERUSEbeforeYouInfuse .
youtu.be/HGtBMHXUVyA?...
Prefer SIRSI
“Somewhat indolent rapid sequence induction”
“Somewhat indolent rapid sequence induction”
I'm here Nick. Sadly I agree with all your points.
On the use of TCI in RSI : guilty as charged.
In my defence I have never called it 'TIVA RSI' and will even concede that maybe I should stop calling it a 'modified RSI'.
It's a SRSI (Somewhat Rapid Sequence Induction).
On the use of TCI in RSI : guilty as charged.
In my defence I have never called it 'TIVA RSI' and will even concede that maybe I should stop calling it a 'modified RSI'.
It's a SRSI (Somewhat Rapid Sequence Induction).
April 19, 2025 at 10:49 PM
Prefer SIRSI
“Somewhat indolent rapid sequence induction”
“Somewhat indolent rapid sequence induction”
Yesssssss!
Anyone using TCI pumps to deliver induction agents during RSI, doesn’t understand the most basic principles of the technique.
bsky.app/profile/chri...
bsky.app/profile/chri...
And the answer is 'No'.
Even at 6 x the maximum infusion rate of a TCI pump the time taken to administer a bolus IV induction agent is still significantly slower than that for a manual bolus during RSI.
bsky.app/profile/simt...
I'm also officially banning use of the idiot term "TIVA RSI".
Even at 6 x the maximum infusion rate of a TCI pump the time taken to administer a bolus IV induction agent is still significantly slower than that for a manual bolus during RSI.
bsky.app/profile/simt...
I'm also officially banning use of the idiot term "TIVA RSI".
April 19, 2025 at 10:47 PM
Yesssssss!
Reposted by Tim Leeuwenburg

We need to make sure GPs can deliver high-quality care sustainably and aren't under pressure to see more people, more quickly.
More targeted funding to support people with chronic, complex conditions is still the most cost-effective way to improve our health system. 3/3
More targeted funding to support people with chronic, complex conditions is still the most cost-effective way to improve our health system. 3/3
RACGP - RACGP applauds GP workforce commitment in Government’s $8.5 billion Medicare package
The Royal Australian College of GPs (RACGP) has applauded the Government’s workforce commitment to train 2,000 new GPs every year by 2028 and incentivise more junior doctors to become specialist GPs, ...
www.racgp.org.au
February 23, 2025 at 9:18 AM
We need to make sure GPs can deliver high-quality care sustainably and aren't under pressure to see more people, more quickly.
More targeted funding to support people with chronic, complex conditions is still the most cost-effective way to improve our health system. 3/3
More targeted funding to support people with chronic, complex conditions is still the most cost-effective way to improve our health system. 3/3
Reposted by Tim Leeuwenburg
That'll need careful consideration to make sure it's sustainable and funding goes to those who need it most.
Extending bulk billing incentives to everyone won't necessarily mean everyone gets bulk billed, because patients' rebates are still too low to cover the cost of care. 2/3
Extending bulk billing incentives to everyone won't necessarily mean everyone gets bulk billed, because patients' rebates are still too low to cover the cost of care. 2/3
February 23, 2025 at 9:18 AM
That'll need careful consideration to make sure it's sustainable and funding goes to those who need it most.
Extending bulk billing incentives to everyone won't necessarily mean everyone gets bulk billed, because patients' rebates are still too low to cover the cost of care. 2/3
Extending bulk billing incentives to everyone won't necessarily mean everyone gets bulk billed, because patients' rebates are still too low to cover the cost of care. 2/3
Reposted by Tim Leeuwenburg

Would like to congratulate my Junior Doctor Colleagues at Hunter New England Local Health District in NSW
Who have recently been appointed as clinical marshmallows.
www.reddit.com/r/ausjdocs/c...
Who have recently been appointed as clinical marshmallows.
www.reddit.com/r/ausjdocs/c...

From the ausjdocs community on Reddit: Supposedly accidentally sent to Hunter New England JMOs…
Explore this post and more from the ausjdocs community
www.reddit.com
January 30, 2025 at 7:49 AM
Would like to congratulate my Junior Doctor Colleagues at Hunter New England Local Health District in NSW
Who have recently been appointed as clinical marshmallows.
www.reddit.com/r/ausjdocs/c...
Who have recently been appointed as clinical marshmallows.
www.reddit.com/r/ausjdocs/c...
Reposted by Tim Leeuwenburg

Now that's a headline.

I knew one day I’d have to watch powerful men burn the world down – I just didn’t expect them to be such losers | Rebecca Shaw
Elon Musk and Mark Zuckerberg’s desperation to be cool as they suck up to Donald Trump is so cringe it makes my skin crawl
www.theguardian.com
January 17, 2025 at 6:13 AM
Now that's a headline.
Hey folks
Meet @shorty-med.bsky.social
A legend in UK paramedicine and prehospital care
And a thoroughly nice chap to boot
Give him a follow for entertaining tidbits on paramedicine and prehospital pearls
Meet @shorty-med.bsky.social
A legend in UK paramedicine and prehospital care
And a thoroughly nice chap to boot
Give him a follow for entertaining tidbits on paramedicine and prehospital pearls
January 16, 2025 at 8:15 AM
Hey folks
Meet @shorty-med.bsky.social
A legend in UK paramedicine and prehospital care
And a thoroughly nice chap to boot
Give him a follow for entertaining tidbits on paramedicine and prehospital pearls
Meet @shorty-med.bsky.social
A legend in UK paramedicine and prehospital care
And a thoroughly nice chap to boot
Give him a follow for entertaining tidbits on paramedicine and prehospital pearls
Reposted by Tim Leeuwenburg

Good to see @anzca.bsky.social continuing to lead the way and move from Twitter/ X to this platform.
This is the new home of medical information on social media.
@AnSky @MedSky
This is the new home of medical information on social media.
@AnSky @MedSky
January 15, 2025 at 8:12 AM
Good to see @anzca.bsky.social continuing to lead the way and move from Twitter/ X to this platform.
This is the new home of medical information on social media.
@AnSky @MedSky
This is the new home of medical information on social media.
@AnSky @MedSky
Benefits of physician-paramedic for prehospital critical care demonstrated in this neat study
www.youtube.com/watch?app=de...
In geographically vast Australia it takes time for teams to arrive to rural/remote incidents
We need rural responder networks to support ambulance in rural Oz
www.youtube.com/watch?app=de...
In geographically vast Australia it takes time for teams to arrive to rural/remote incidents
We need rural responder networks to support ambulance in rural Oz

Benefits of physician-paramedic interprofessional pre-hospital teams
YouTube video by Mike Christian
www.youtube.com
January 7, 2025 at 9:41 PM
Benefits of physician-paramedic for prehospital critical care demonstrated in this neat study
www.youtube.com/watch?app=de...
In geographically vast Australia it takes time for teams to arrive to rural/remote incidents
We need rural responder networks to support ambulance in rural Oz
www.youtube.com/watch?app=de...
In geographically vast Australia it takes time for teams to arrive to rural/remote incidents
We need rural responder networks to support ambulance in rural Oz
Today has been a day for possum care here on Kangaroo Island
Spending my anaesthetic oncall caring for native wildlife….
Spending my anaesthetic oncall caring for native wildlife….


January 3, 2025 at 7:48 AM
Today has been a day for possum care here on Kangaroo Island
Spending my anaesthetic oncall caring for native wildlife….
Spending my anaesthetic oncall caring for native wildlife….
60 public access defibrillators on Kangaroo Island (South Australia) under the HeartSafeKI program - along with 30% of island population (4200) trained in hands only CPR - included under SA Ambulance and @goodsamapp.bsky.social
60 people blocked c access defibrillators on Kangaroo Island (South Australia) under the HeartSafeKI program - along with 30% of island population (4200) trained in hands only CPR - included under SA Ambulance and @goodsamapp.bsky.social

Christmas holiday challenge for you! Just been on a run and saw at least 5 defibrillators. How many @gwaac.bsky.social or other defibrillators can you see? These might one day save the life of someone you know.
These ones provided by our local air ambulance
#defibrillator #heartstarter
These ones provided by our local air ambulance
#defibrillator #heartstarter
December 24, 2024 at 10:44 PM
60 public access defibrillators on Kangaroo Island (South Australia) under the HeartSafeKI program - along with 30% of island population (4200) trained in hands only CPR - included under SA Ambulance and @goodsamapp.bsky.social
60 people blocked c access defibrillators on Kangaroo Island (South Australia) under the HeartSafeKI program - along with 30% of island population (4200) trained in hands only CPR - included under SA Ambulance and @goodsamapp.bsky.social
Christmas holiday challenge for you! Just been on a run and saw at least 5 defibrillators. How many @gwaac.bsky.social or other defibrillators can you see? These might one day save the life of someone you know.
These ones provided by our local air ambulance
#defibrillator #heartstarter
These ones provided by our local air ambulance
#defibrillator #heartstarter
December 24, 2024 at 10:44 AM
60 people blocked c access defibrillators on Kangaroo Island (South Australia) under the HeartSafeKI program - along with 30% of island population (4200) trained in hands only CPR - included under SA Ambulance and @goodsamapp.bsky.social