



Policy Sketchbook
@policysketch.bsky.social
Possible my memory is failing me, but I feel like it's a while since I saw one of these charts shaped like this, because it's a while since we meaningfully increased benefits - which is the only way to support the lowest income groups, who pay very little in tax, so don't benefit from tax cuts.

How has the Budget impacted living standards? The distributional impact of all tax/benefit changes since Autumn Budget 2024 is progressive:poorer households gain from 2-child limit repeal and UC boost, while richer households lose from threshold freezes and new property, dividend and savings taxes

November 27, 2025 at 2:01 PM
Possible my memory is failing me, but I feel like it's a while since I saw one of these charts shaped like this, because it's a while since we meaningfully increased benefits - which is the only way to support the lowest income groups, who pay very little in tax, so don't benefit from tax cuts.
Reposted by Policy Sketchbook
This SUNDAY - COLCHESTER!!
A solo show for @samaritans.bsky.social
Tickets here
www.redlionbooks.co.uk/product/poet...
Tell your friends
A solo show for @samaritans.bsky.social
Tickets here
www.redlionbooks.co.uk/product/poet...
Tell your friends
November 22, 2025 at 10:48 AM
This SUNDAY - COLCHESTER!!
A solo show for @samaritans.bsky.social
Tickets here
www.redlionbooks.co.uk/product/poet...
Tell your friends
A solo show for @samaritans.bsky.social
Tickets here
www.redlionbooks.co.uk/product/poet...
Tell your friends
For 90% of people there is no good reason these days to own a high value phone when a second hand one from several years ago can do everything you need it to and more. The added bonus appears to be that would-be muggers won't want to take it from you.

The brutal reality of life as an Android owner in London: First you’re shocked as you’re mugged. Then you’re humiliated as the thief returns the device. www.londoncentric.media/p/london-pho...

"Don't want no Samsung"
Plus: Scroll down to see what might be the strangest new artwork in the capital and read more on our investigations into the capital's landlords.
www.londoncentric.media
November 18, 2025 at 9:53 AM
For 90% of people there is no good reason these days to own a high value phone when a second hand one from several years ago can do everything you need it to and more. The added bonus appears to be that would-be muggers won't want to take it from you.
[the sound of a million people searching for HotDogGuy.jpg]

November 18, 2025 at 8:56 AM
[the sound of a million people searching for HotDogGuy.jpg]
Reposted by Policy Sketchbook

New post just out:
"On the edge"
On my unexpected week in hospital and five things I learnt about the state of the NHS.
(Free to read)
open.substack.com/pub/samf/p/o...
"On the edge"
On my unexpected week in hospital and five things I learnt about the state of the NHS.
(Free to read)
open.substack.com/pub/samf/p/o...

On the edge
My week in the NHS
open.substack.com
October 19, 2025 at 8:14 AM
New post just out:
"On the edge"
On my unexpected week in hospital and five things I learnt about the state of the NHS.
(Free to read)
open.substack.com/pub/samf/p/o...
"On the edge"
On my unexpected week in hospital and five things I learnt about the state of the NHS.
(Free to read)
open.substack.com/pub/samf/p/o...
It's almost like... this is the point of a narrow tax base and heavily means-tested benefits.

And ofc governments themselves have significant influence over how much tax people pay
George Osborne bragged that his decision to raise the personal allowance meant loads of low-income people wouldn't pay income tax
Years later, that became a stick to beat them samf.substack.com/p/the-someth...
George Osborne bragged that his decision to raise the personal allowance meant loads of low-income people wouldn't pay income tax
Years later, that became a stick to beat them samf.substack.com/p/the-someth...

October 17, 2025 at 1:26 PM
It's almost like... this is the point of a narrow tax base and heavily means-tested benefits.
Reposted by Policy Sketchbook

It's been a rough two decades for non-pensioner real income growth after housing costs, especially for the poorest households. www.resolutionfoundation.org/publications...

September 18, 2025 at 8:26 AM
It's been a rough two decades for non-pensioner real income growth after housing costs, especially for the poorest households. www.resolutionfoundation.org/publications...
Reposted by Policy Sketchbook

You do, but most analysis suggests this is massively outweighed by cost increases from technology. Some helpful discussion from @policysketch.bsky.social here policysketchbook.wordpress.com/2018/01/06/p...

Prevention, longevity and health system costs
Kailash Chand has a piece in the Guardian arguing that unless the NHS fundamentally changes its approach to focus on prevention rather than cure, it will not be financially sustainable. This remind…
policysketchbook.wordpress.com
August 31, 2025 at 9:25 AM
You do, but most analysis suggests this is massively outweighed by cost increases from technology. Some helpful discussion from @policysketch.bsky.social here policysketchbook.wordpress.com/2018/01/06/p...
The obvious conclusion from this article is "don't use age verification yet unless you absolutely have to". It's in its chaotic infancy and will probably be much safer at some point in the future.
www.pcgamer.com/hardware/the...
www.pcgamer.com/hardware/the...

The UK's new age verification is a privacy nightmare, but it doesn't need to be
"They are over exposing data to prove a simple point, but there are ample alternatives."
www.pcgamer.com
August 3, 2025 at 8:54 AM
The obvious conclusion from this article is "don't use age verification yet unless you absolutely have to". It's in its chaotic infancy and will probably be much safer at some point in the future.
www.pcgamer.com/hardware/the...
www.pcgamer.com/hardware/the...
Reposted by Policy Sketchbook

Reposted by Policy Sketchbook
Policy exchange, backed by Sajid Javid, think we need to switch the NHS funding model to social insurance, and introduce new charges for NHS services, like to see a GP
policyexchange.org.uk/publication/...
These are not new ideas, but they are bad ideas
A thread with some evidence
policyexchange.org.uk/publication/...
These are not new ideas, but they are bad ideas
A thread with some evidence

The NHS – a Suitable Case for Treatment? - Policy Exchange
Download Publication Online Reader ‘The NHS – a Suitable Case for Treatment?’ makes the case that the NHS is not fit for purpose and is in urgent need of reform.The report finds that NHS performance r...
policyexchange.org.uk
July 23, 2025 at 8:06 PM
Policy exchange, backed by Sajid Javid, think we need to switch the NHS funding model to social insurance, and introduce new charges for NHS services, like to see a GP
policyexchange.org.uk/publication/...
These are not new ideas, but they are bad ideas
A thread with some evidence
policyexchange.org.uk/publication/...
These are not new ideas, but they are bad ideas
A thread with some evidence
Have to wonder how much of an issue is that we hold the chief accountant responsible for economic growth. Accountancy and growth are really not the same thing!

"For all her efforts, however, Reeves’ Mansion House announcements are unlikely to shift the dial on the UK’s downbeat growth prospects"
She might as well be doing a weather dance.
She might as well be doing a weather dance.

Rachel Reeves’ limited pitch to Britain’s financial sector https://on.ft.com/4eTdXei | opinion
July 16, 2025 at 10:54 AM
Have to wonder how much of an issue is that we hold the chief accountant responsible for economic growth. Accountancy and growth are really not the same thing!
The fact that Bluesky is, as far as most people will care, a functionally identical app to Twitter, but even a Nazi chatbot doesn't shift user numbers across, is a pretty strong demonstration of the power of network effects in generating social media monopolies.
July 8, 2025 at 10:43 PM
The fact that Bluesky is, as far as most people will care, a functionally identical app to Twitter, but even a Nazi chatbot doesn't shift user numbers across, is a pretty strong demonstration of the power of network effects in generating social media monopolies.
Reposted by Policy Sketchbook

The "welfare spending out of control" narrative is nonsense.
But this chart tells us almost nothing. Not comparing like-with-like ("social protection" ≠ DWP welfare spend).
And most of the difference driven by fact UK has (private) occupational pensions, other countries have state schemes
But this chart tells us almost nothing. Not comparing like-with-like ("social protection" ≠ DWP welfare spend).
And most of the difference driven by fact UK has (private) occupational pensions, other countries have state schemes

The entire UK political/media narrative on welfare is that it is "burgeoning", "a burden" & "unsustainable". But how high is it compared to others? UK welfare at 10.8% of GDP in 2023 (including pensions). Finland spends 25.7% of GDP; France 23.8%: both double the UK.

July 6, 2025 at 9:48 AM
The "welfare spending out of control" narrative is nonsense.
But this chart tells us almost nothing. Not comparing like-with-like ("social protection" ≠ DWP welfare spend).
And most of the difference driven by fact UK has (private) occupational pensions, other countries have state schemes
But this chart tells us almost nothing. Not comparing like-with-like ("social protection" ≠ DWP welfare spend).
And most of the difference driven by fact UK has (private) occupational pensions, other countries have state schemes
Reposted by Policy Sketchbook

Didn't promote my latest properly, so, yeah - NEW BLOGPOST
Basically, Britain is bad at management, it's fucking our economy, and politicians and journalists don't address it because they are the worst exemplars of it.
www.joxleywrites.jmoxley.co.uk/p/britain-ca...
Basically, Britain is bad at management, it's fucking our economy, and politicians and journalists don't address it because they are the worst exemplars of it.
www.joxleywrites.jmoxley.co.uk/p/britain-ca...

Britain can't manage like this
A cultural aversion to management is undermining our economy
www.joxleywrites.jmoxley.co.uk
June 27, 2025 at 7:51 PM
Didn't promote my latest properly, so, yeah - NEW BLOGPOST
Basically, Britain is bad at management, it's fucking our economy, and politicians and journalists don't address it because they are the worst exemplars of it.
www.joxleywrites.jmoxley.co.uk/p/britain-ca...
Basically, Britain is bad at management, it's fucking our economy, and politicians and journalists don't address it because they are the worst exemplars of it.
www.joxleywrites.jmoxley.co.uk/p/britain-ca...
Reposted by Policy Sketchbook

The OBR enhances the power of the chancellor by giving them more tools to push their preferences onto other departments, rather than undermining elected politicians. Truss and Kwarteng were simply bad at this game.
June 11, 2025 at 7:35 AM
The OBR enhances the power of the chancellor by giving them more tools to push their preferences onto other departments, rather than undermining elected politicians. Truss and Kwarteng were simply bad at this game.
I think my view on this is that we should absolutely recognise that people struggle to assimilate the information they get from various sources and do indeed end up with skewed opinions as a result. But we should also be very sceptical of our own abilities to avoid these pitfalls.

Second, a view that the masses are merely subjects whose own views never come from their own observations and experiences but rather from what they are told to believe. Funnily enough, proponents of this view always imagine themselves to be immune from similar forces.
May 15, 2025 at 5:22 PM
I think my view on this is that we should absolutely recognise that people struggle to assimilate the information they get from various sources and do indeed end up with skewed opinions as a result. But we should also be very sceptical of our own abilities to avoid these pitfalls.
Reposted by Policy Sketchbook

A great example of using (very) small area geographies to generate headline-grabbing statistics. Bradford Central is a mid-level super output area, one of 63 in the Bradford local authority area. It accounts for 1.2% of the population. 81% of Bradford residents were born in the UK (Census 2021).

🚨 NEW: Robert Jenrick backs PM with claim UK already an ‘island of strangers’ in some places
“Aggressive levels of mass migration have made us more divided... for example central Bradford - 50 per cent of people were born outside of the UK”, he said
Full story ⤵️
www.politics.co.uk/news/2025/05...
“Aggressive levels of mass migration have made us more divided... for example central Bradford - 50 per cent of people were born outside of the UK”, he said
Full story ⤵️
www.politics.co.uk/news/2025/05...

Robert Jenrick backs PM with claim UK already an ‘island of strangers’ in some places - Politics.co.uk
Keir Starmer has faced a backlash after he said the UK risked becoming an island of strangers if migration remained unchecked.
www.politics.co.uk
May 13, 2025 at 6:27 PM
A great example of using (very) small area geographies to generate headline-grabbing statistics. Bradford Central is a mid-level super output area, one of 63 in the Bradford local authority area. It accounts for 1.2% of the population. 81% of Bradford residents were born in the UK (Census 2021).
I do not want to vote for a party led by a former hypnotist (breast-related or otherwise) but also we elected the sensible guy with the impeccable CV and now he has gone hard right on immigration rhetoric so where do we go now?
May 13, 2025 at 8:19 AM
I do not want to vote for a party led by a former hypnotist (breast-related or otherwise) but also we elected the sensible guy with the impeccable CV and now he has gone hard right on immigration rhetoric so where do we go now?
Reposted by Policy Sketchbook

a society where "bad immigrants" are demonised is a society where no immigrant can truly feel welcome, because aren't we all just one wrong turn or accident away from being unemployed? on disability benefits? unable to care for our children without state help? just no such thing as a safe immigrant
May 12, 2025 at 12:19 PM
a society where "bad immigrants" are demonised is a society where no immigrant can truly feel welcome, because aren't we all just one wrong turn or accident away from being unemployed? on disability benefits? unable to care for our children without state help? just no such thing as a safe immigrant
Reposted by Policy Sketchbook

For those who voted Labour in 2024 immigration (5%) was behind The Economy (49%), Health (19%), Environment (8%) and Inequality (7%) in their most important issues. /3
May 12, 2025 at 10:12 AM
For those who voted Labour in 2024 immigration (5%) was behind The Economy (49%), Health (19%), Environment (8%) and Inequality (7%) in their most important issues. /3
Reposted by Policy Sketchbook

An excellent summary of why Labour is doomed and will simply open the door to Farage and his outriders. As Wilson famously remarked, the Labour Party is a moral crusade, or it is nothing. Looks like they've made their choice
Since they aren’t real problems (at least as described) they of course can’t be solved by the policies Labour are pursuing. So the government will look like a failure, the grievances will remain and there will be demands to go further.
May 11, 2025 at 5:46 PM
An excellent summary of why Labour is doomed and will simply open the door to Farage and his outriders. As Wilson famously remarked, the Labour Party is a moral crusade, or it is nothing. Looks like they've made their choice
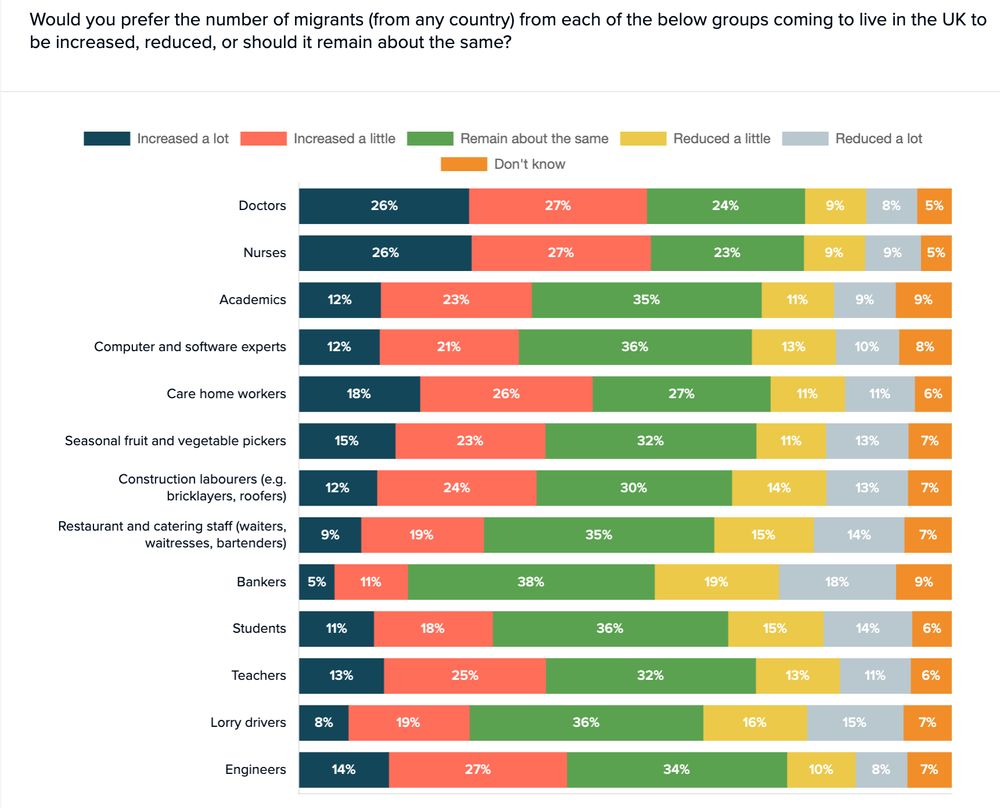
It follows that Labour are governing on behalf of the 20% of voters who want immigration from pretty much all professional groups reduced, and to hell with the other 80% of us.

What would public choose on social care workers coming to Britain?
Increase the numbers: 44% (18% a lot, 26% a little)
Maintain current levels: 27%
Reduce the numbers: 22% (11% reduce a lot, 11% a little)
Focaldata for British Future (2nd - 6th May 2025)
www.britishfuture.org/white-paper-...
Increase the numbers: 44% (18% a lot, 26% a little)
Maintain current levels: 27%
Reduce the numbers: 22% (11% reduce a lot, 11% a little)
Focaldata for British Future (2nd - 6th May 2025)
www.britishfuture.org/white-paper-...
May 11, 2025 at 3:47 PM
It follows that Labour are governing on behalf of the 20% of voters who want immigration from pretty much all professional groups reduced, and to hell with the other 80% of us.
We are stuck in a loop of politicians promising us whatever we want, with no trade-offs, because everyone is scared that if they admit to the downsides, someone else will "outflank" them by promising all the good stuff with no drawbacks.
May 8, 2025 at 8:33 AM
We are stuck in a loop of politicians promising us whatever we want, with no trade-offs, because everyone is scared that if they admit to the downsides, someone else will "outflank" them by promising all the good stuff with no drawbacks.