



Anoushka Dua MD
@anoushkaduamd.bsky.social
2nd Year GI fellow at UC Irvine by way of UCLA Internal Med 💙💛 #WomeninGI ACG Women in GI Committee | ACG EBGI ambassador | views = my own
YES!!!! Let’s encourage everyone else too!
April 4, 2025 at 10:47 PM
YES!!!! Let’s encourage everyone else too!
Thank you for sharing this! Absolutely agree that we need to do better in not remaining siloed in our specialties. Multiple cancers over multiple generations = red flag!
March 25, 2025 at 4:54 PM
Thank you for sharing this! Absolutely agree that we need to do better in not remaining siloed in our specialties. Multiple cancers over multiple generations = red flag!
March 19, 2025 at 2:17 AM
11/
References📄:
1. bit.ly/3RdSnpA
2. bit.ly/3FKSRky
3. bit.ly/4bxcAQR, bit.ly/42bmcgR
4. bit.ly/4iBxnoH, bit.ly/4hEie4T
References📄:
1. bit.ly/3RdSnpA
2. bit.ly/3FKSRky
3. bit.ly/4bxcAQR, bit.ly/42bmcgR
4. bit.ly/4iBxnoH, bit.ly/4hEie4T
March 19, 2025 at 2:17 AM
11/
References📄:
1. bit.ly/3RdSnpA
2. bit.ly/3FKSRky
3. bit.ly/4bxcAQR, bit.ly/42bmcgR
4. bit.ly/4iBxnoH, bit.ly/4hEie4T
References📄:
1. bit.ly/3RdSnpA
2. bit.ly/3FKSRky
3. bit.ly/4bxcAQR, bit.ly/42bmcgR
4. bit.ly/4iBxnoH, bit.ly/4hEie4T
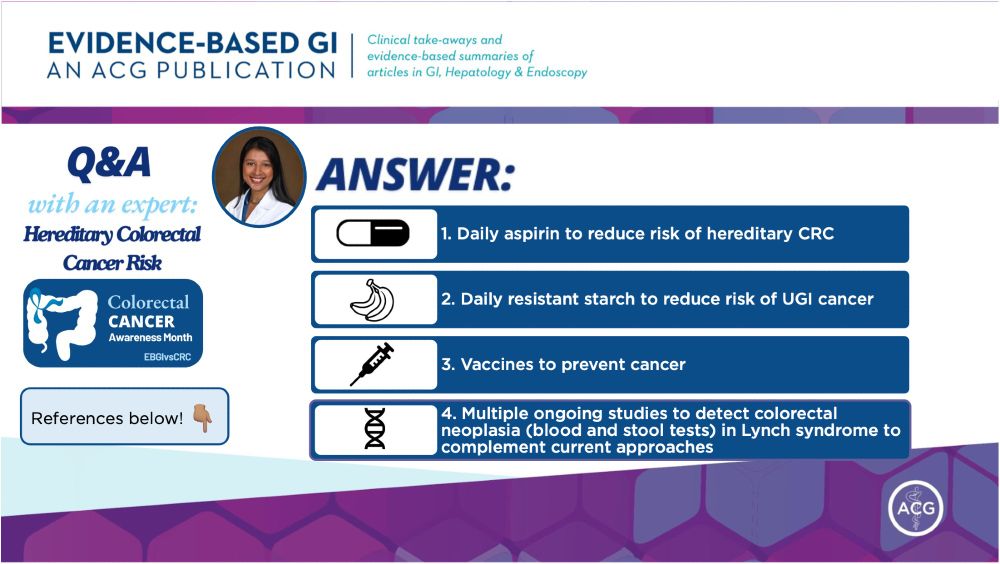
10/
Q5: What are some of the latest advancements in the treatment of hereditary colorectal cancer syndromes?
#Gastrosky
Q5: What are some of the latest advancements in the treatment of hereditary colorectal cancer syndromes?
#Gastrosky
March 19, 2025 at 2:17 AM
10/
Q5: What are some of the latest advancements in the treatment of hereditary colorectal cancer syndromes?
#Gastrosky
Q5: What are some of the latest advancements in the treatment of hereditary colorectal cancer syndromes?
#Gastrosky
9/
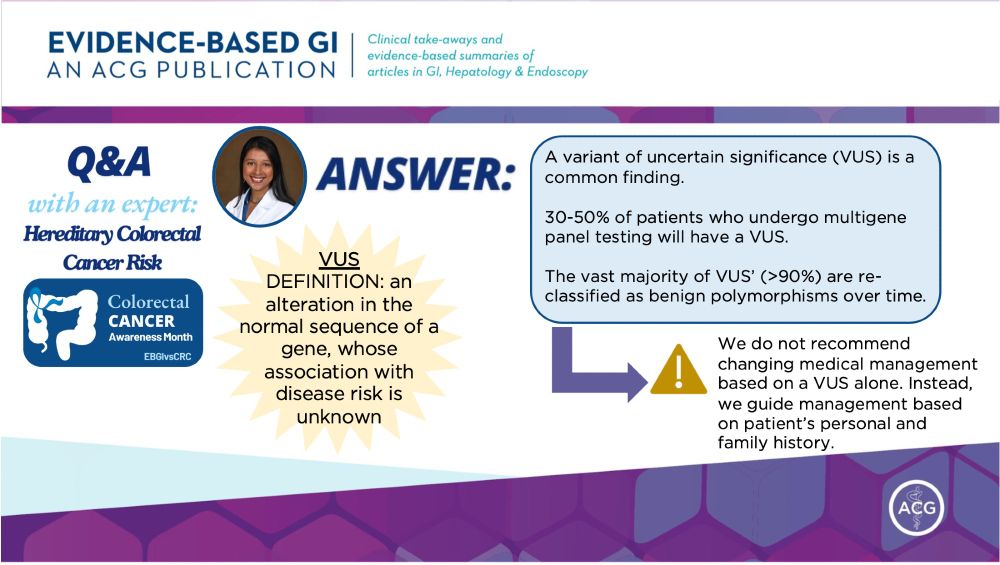
VUS: genetic alteration w/ unknown disease risk
🧬 Common, found in 30-50% of patients undergoing multigene panel testing
🧬 >90% of VUS are re-classified as benign over ⏰
⚠️ Do 🚫 recommend changing medical management based on VUS alone!
VUS: genetic alteration w/ unknown disease risk
🧬 Common, found in 30-50% of patients undergoing multigene panel testing
🧬 >90% of VUS are re-classified as benign over ⏰
⚠️ Do 🚫 recommend changing medical management based on VUS alone!
March 19, 2025 at 2:17 AM
9/
VUS: genetic alteration w/ unknown disease risk
🧬 Common, found in 30-50% of patients undergoing multigene panel testing
🧬 >90% of VUS are re-classified as benign over ⏰
⚠️ Do 🚫 recommend changing medical management based on VUS alone!
VUS: genetic alteration w/ unknown disease risk
🧬 Common, found in 30-50% of patients undergoing multigene panel testing
🧬 >90% of VUS are re-classified as benign over ⏰
⚠️ Do 🚫 recommend changing medical management based on VUS alone!
8/
Q4: What are the implications of identifying a ”variant of uncertain significance” on genetic testing🧬?
#Gastrosky
Q4: What are the implications of identifying a ”variant of uncertain significance” on genetic testing🧬?
#Gastrosky
March 19, 2025 at 2:17 AM
8/
Q4: What are the implications of identifying a ”variant of uncertain significance” on genetic testing🧬?
#Gastrosky
Q4: What are the implications of identifying a ”variant of uncertain significance” on genetic testing🧬?
#Gastrosky
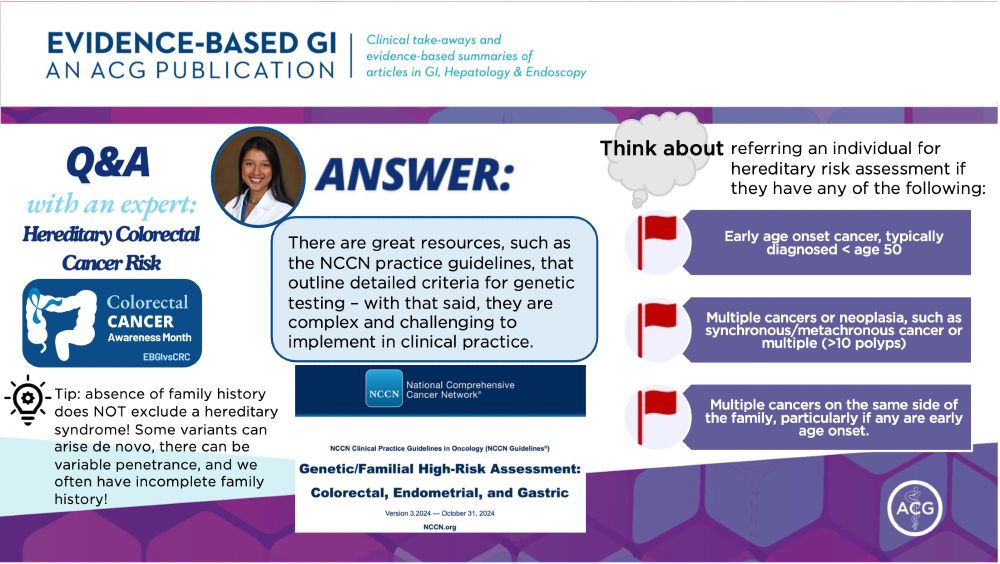
7/
NCCN guidelines excellent but complex 👇🏽
bit.ly/4iQwTei
Broadly speaking, think about referring if:
🔎 Early onset cancer age < 50
🔎 Multiple cancers or >10 polyps
🔎 Multiple cancers on same side of family
Note: absence of family hx does not 🚫 a hereditary syndrome!
NCCN guidelines excellent but complex 👇🏽
bit.ly/4iQwTei
Broadly speaking, think about referring if:
🔎 Early onset cancer age < 50
🔎 Multiple cancers or >10 polyps
🔎 Multiple cancers on same side of family
Note: absence of family hx does not 🚫 a hereditary syndrome!
March 19, 2025 at 2:17 AM
7/
NCCN guidelines excellent but complex 👇🏽
bit.ly/4iQwTei
Broadly speaking, think about referring if:
🔎 Early onset cancer age < 50
🔎 Multiple cancers or >10 polyps
🔎 Multiple cancers on same side of family
Note: absence of family hx does not 🚫 a hereditary syndrome!
NCCN guidelines excellent but complex 👇🏽
bit.ly/4iQwTei
Broadly speaking, think about referring if:
🔎 Early onset cancer age < 50
🔎 Multiple cancers or >10 polyps
🔎 Multiple cancers on same side of family
Note: absence of family hx does not 🚫 a hereditary syndrome!
6/
Q3: In what clinical scenarios should gastroenterology providers think about referring patients for genetic testing🧬?
#Gastrosky
Q3: In what clinical scenarios should gastroenterology providers think about referring patients for genetic testing🧬?
#Gastrosky
March 19, 2025 at 2:17 AM
6/
Q3: In what clinical scenarios should gastroenterology providers think about referring patients for genetic testing🧬?
#Gastrosky
Q3: In what clinical scenarios should gastroenterology providers think about referring patients for genetic testing🧬?
#Gastrosky
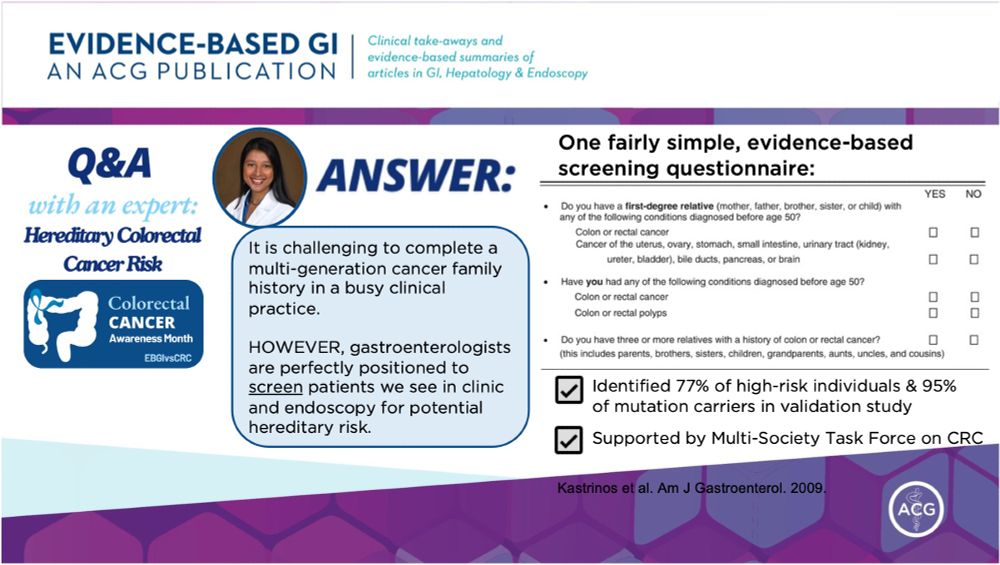
5/
📝Simple 3Q screening tool (Kastrinos et al. 2009) is feasible!
1. FDR < 50 with CRC, CA of uterus, ovary, stomach, small intestine, urinary tract, bile duct, pancreas, brain?
2. CRC or polyps at age < 50?
3. 3+ relatives w/ CRC?
✅High sensitivity
✅Supported by MSTF on CRC
📝Simple 3Q screening tool (Kastrinos et al. 2009) is feasible!
1. FDR < 50 with CRC, CA of uterus, ovary, stomach, small intestine, urinary tract, bile duct, pancreas, brain?
2. CRC or polyps at age < 50?
3. 3+ relatives w/ CRC?
✅High sensitivity
✅Supported by MSTF on CRC
March 19, 2025 at 2:17 AM
5/
📝Simple 3Q screening tool (Kastrinos et al. 2009) is feasible!
1. FDR < 50 with CRC, CA of uterus, ovary, stomach, small intestine, urinary tract, bile duct, pancreas, brain?
2. CRC or polyps at age < 50?
3. 3+ relatives w/ CRC?
✅High sensitivity
✅Supported by MSTF on CRC
📝Simple 3Q screening tool (Kastrinos et al. 2009) is feasible!
1. FDR < 50 with CRC, CA of uterus, ovary, stomach, small intestine, urinary tract, bile duct, pancreas, brain?
2. CRC or polyps at age < 50?
3. 3+ relatives w/ CRC?
✅High sensitivity
✅Supported by MSTF on CRC
4/
Q2: What are the key elements of a family history that should be collected to assess the risk of hereditary colorectal cancer?
#Gastrosky
Q2: What are the key elements of a family history that should be collected to assess the risk of hereditary colorectal cancer?
#Gastrosky
March 19, 2025 at 2:17 AM
4/
Q2: What are the key elements of a family history that should be collected to assess the risk of hereditary colorectal cancer?
#Gastrosky
Q2: What are the key elements of a family history that should be collected to assess the risk of hereditary colorectal cancer?
#Gastrosky
3/
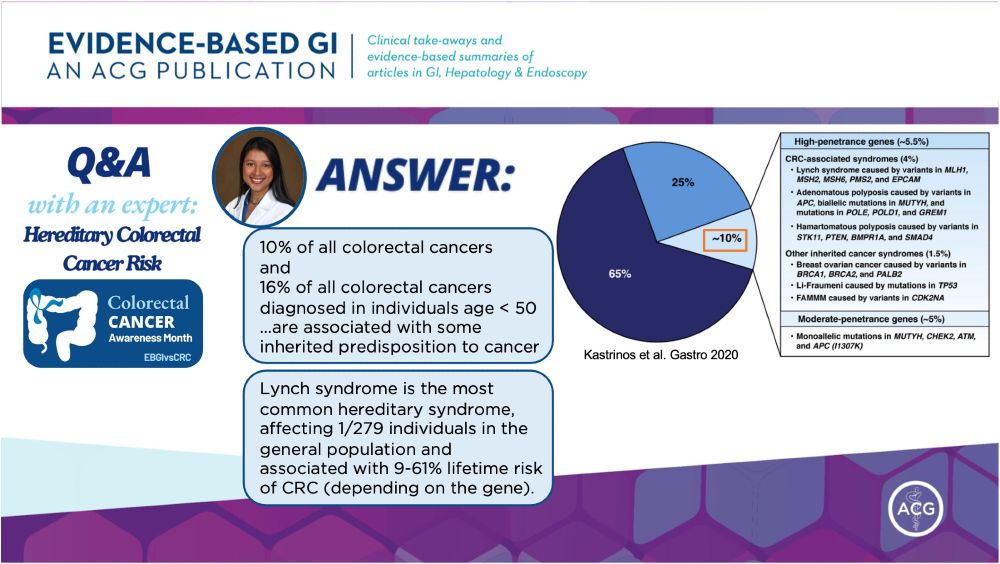
Hereditary CRC makes up:
🔹10% of all CRC
🔹16% of all CRC in age < 50
Most common: Lynch syndrome
Caused by:
🧬MMR gene mutations including MLH1, MSH2, MSH6, PMS2
or
🧬EPCAM mutation which sits upstream of MSH2)
Prevalence: 1/279 individuals in general population👥
Hereditary CRC makes up:
🔹10% of all CRC
🔹16% of all CRC in age < 50
Most common: Lynch syndrome
Caused by:
🧬MMR gene mutations including MLH1, MSH2, MSH6, PMS2
or
🧬EPCAM mutation which sits upstream of MSH2)
Prevalence: 1/279 individuals in general population👥
March 19, 2025 at 2:17 AM
3/
Hereditary CRC makes up:
🔹10% of all CRC
🔹16% of all CRC in age < 50
Most common: Lynch syndrome
Caused by:
🧬MMR gene mutations including MLH1, MSH2, MSH6, PMS2
or
🧬EPCAM mutation which sits upstream of MSH2)
Prevalence: 1/279 individuals in general population👥
Hereditary CRC makes up:
🔹10% of all CRC
🔹16% of all CRC in age < 50
Most common: Lynch syndrome
Caused by:
🧬MMR gene mutations including MLH1, MSH2, MSH6, PMS2
or
🧬EPCAM mutation which sits upstream of MSH2)
Prevalence: 1/279 individuals in general population👥
March 19, 2025 at 2:17 AM