


@atc-ventilator.bsky.social
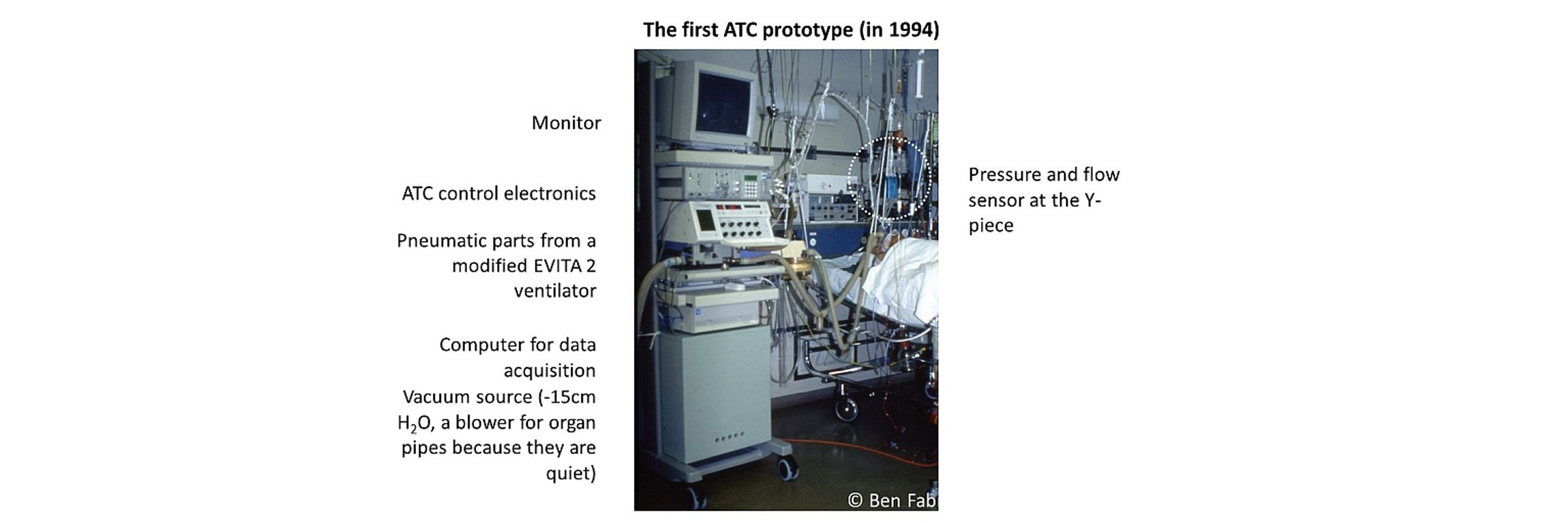
Developed the Automatic Tube Compensation mode (that was my PhD project) in 1993, now Prof. of Physics at Erlangen University (Germany), main research in cellular mechanobiology https://bio.physik.fau.de/
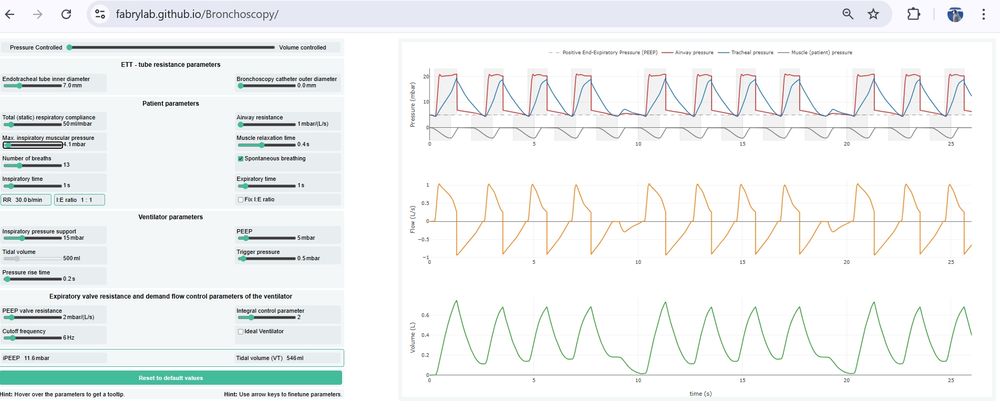
We developed a browser-based tool to predict ventilation impairments such as iPEEP buildup, hypoventilation, and desynchronization due to the tube resistance (also during bronchoscopy). Check it out: fabrylab.github.io/Bronchoscopy/
May 13, 2025 at 8:41 AM
We developed a browser-based tool to predict ventilation impairments such as iPEEP buildup, hypoventilation, and desynchronization due to the tube resistance (also during bronchoscopy). Check it out: fabrylab.github.io/Bronchoscopy/
The flow limitation imposed by the endotracheal tube is a major cause of weaning failure, patient-ventilator desynchronization, and PSILI. During bronchoscopy, the tube resistance becomes prohibitive. Check out our paper medrxiv.org/cgi/content/...

Prediction and Prevention of Ventilation Impairments During Bronchoscopy
Bronchoscopy in mechanically ventilated patients is performed by passing a bronchoscope through the endotracheal tube (ETT), which substantially increases airflow resistance and may compromise ventila...
medrxiv.org
May 13, 2025 at 8:39 AM
The flow limitation imposed by the endotracheal tube is a major cause of weaning failure, patient-ventilator desynchronization, and PSILI. During bronchoscopy, the tube resistance becomes prohibitive. Check out our paper medrxiv.org/cgi/content/...
Empowering patients to breathe spontaneously as early as possible, and only support the work of breathing the patient cannot produce on their own, is the best way to reduce the pressure load on the lungs, and to avoid VILI.
January 15, 2025 at 6:08 PM
Empowering patients to breathe spontaneously as early as possible, and only support the work of breathing the patient cannot produce on their own, is the best way to reduce the pressure load on the lungs, and to avoid VILI.
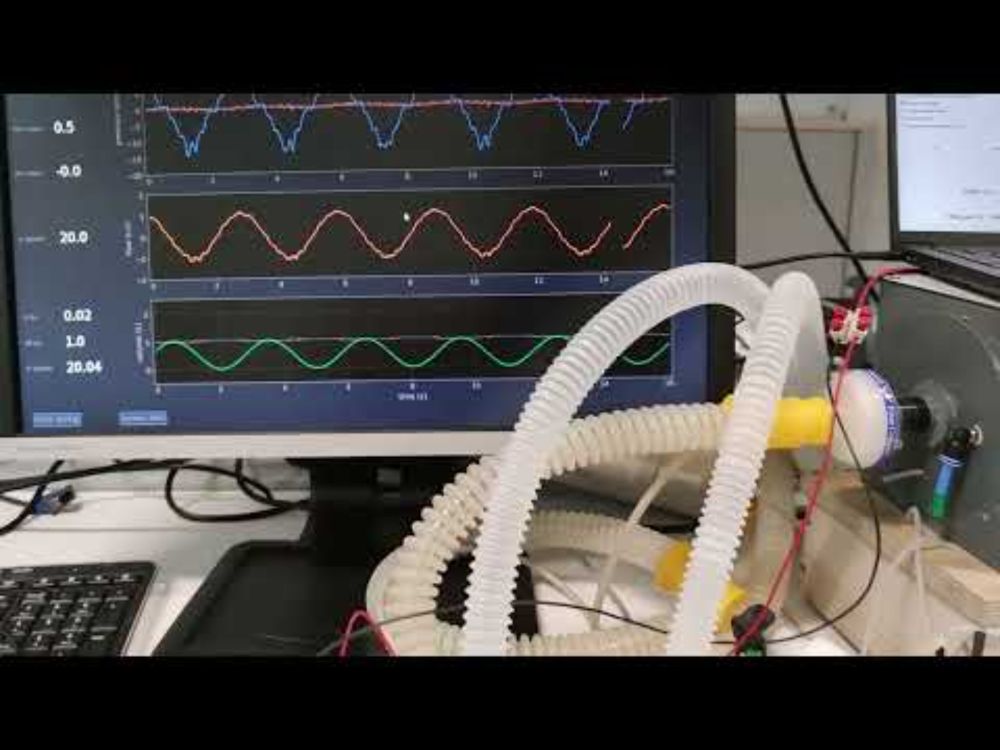
How does a commercial ventilator (Dräger V600) in ATC mode compare to my 3D printed ATC ventilator? Poorly, I would say, but judge for yourself. I am convinced that weaning can be greatly improved and shortened with real ATC. youtu.be/Y4To7-krE14
Comparison ATC-mode Dräger V600 vs self-made ATC ventilator
YouTube video by lpmtvideo
youtu.be
December 20, 2024 at 4:02 PM
How does a commercial ventilator (Dräger V600) in ATC mode compare to my 3D printed ATC ventilator? Poorly, I would say, but judge for yourself. I am convinced that weaning can be greatly improved and shortened with real ATC. youtu.be/Y4To7-krE14
Yesterday, with the retirement symposium of my academic mentor Jeff Fredberg, the era of respiratory physiology research at the Harvard School of Public Health that began with Jim Whittenberger in 1948 came to an end.

December 15, 2024 at 2:37 PM
Yesterday, with the retirement symposium of my academic mentor Jeff Fredberg, the era of respiratory physiology research at the Harvard School of Public Health that began with Jim Whittenberger in 1948 came to an end.
Few of you know that my lab is also active in whale research. That's why I’m urging you to sign the petition to free anti-whaling activist Paul Watson. Denmark may extradite him to Japan, where he faces a 15-year prison sentence. www.paulwatsonfoundation.org/freepaulwats...

The #FREEPAULWATSON petition
On July 21 2024, Captain Paul Watson was arrested by Danish police upon arrival in Nuuk, Greenland, onboard the M/Y John Paul DeJoria. We need your help to #FREEPAULWATSON.
www.paulwatsonfoundation.org
December 10, 2024 at 12:13 PM
Few of you know that my lab is also active in whale research. That's why I’m urging you to sign the petition to free anti-whaling activist Paul Watson. Denmark may extradite him to Japan, where he faces a 15-year prison sentence. www.paulwatsonfoundation.org/freepaulwats...
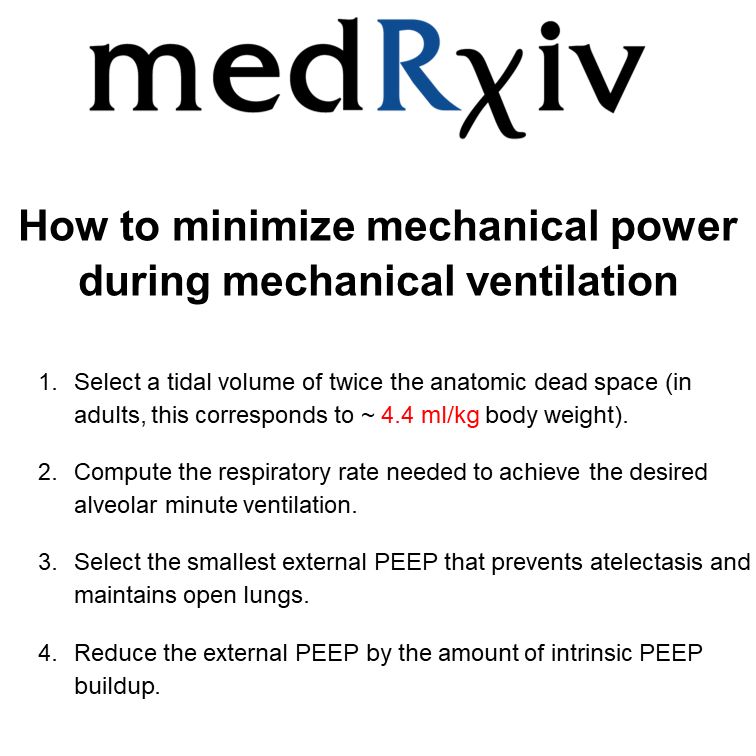
"How to minimize mechanical power during controlled mechanical ventilation" is now published in Int Care Med Exp (doi.org/10.1186/s406...). Main insight: the elastic power is ALWAYS minimized at a VT of twice the anatomic dead space, or ~4.4 ml/kg of body weight.
How to minimize mechanical power during controlled mechanical ventilation - Intensive Care Medicine Experimental
High intrapulmonary pressures, large tidal volumes, and elevated respiratory rates during controlled mechanical ventilation can lead to barotrauma, volutrauma, and atelectrauma. Mechanical power—defin...
doi.org
December 9, 2024 at 1:28 PM
"How to minimize mechanical power during controlled mechanical ventilation" is now published in Int Care Med Exp (doi.org/10.1186/s406...). Main insight: the elastic power is ALWAYS minimized at a VT of twice the anatomic dead space, or ~4.4 ml/kg of body weight.
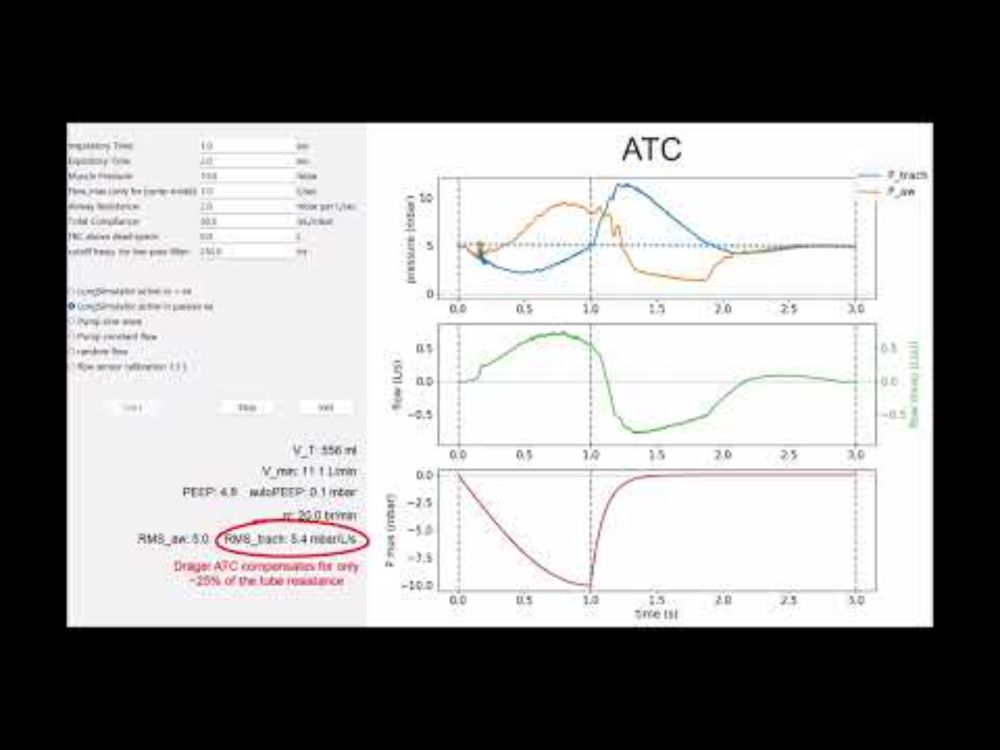
Today, I tested the Dräger Evita V600 ventilator in CPAP and ATC mode with a lung simulator. CPAP worked well, but in ATC mode, the V600 compensates only ~25% of the total tube resistance, and that is possibly not enough to make a difference for patients. youtu.be/AcRkQqnk-gg
Dräger Evita V600 in CPAP and ATC mode
YouTube video by lpmtvideo
youtu.be
December 6, 2024 at 6:55 PM
Today, I tested the Dräger Evita V600 ventilator in CPAP and ATC mode with a lung simulator. CPAP worked well, but in ATC mode, the V600 compensates only ~25% of the total tube resistance, and that is possibly not enough to make a difference for patients. youtu.be/AcRkQqnk-gg
I imported my Twitter posts using Porto (Chrome extension) to add some content. Sorry for cluttering up your timeline. I also have to say that Porto did not work so well, it ignored most of my tweets, for no reason.
December 5, 2024 at 8:19 PM
I imported my Twitter posts using Porto (Chrome extension) to add some content. Sorry for cluttering up your timeline. I also have to say that Porto did not work so well, it ignored most of my tweets, for no reason.
I used to be on Twitter (@ATC_Ventilator) and now join Bluesky; my aim is to discuss topics around the mode Automatic Tube Compensation, weaning, lung physiology and mechanical ventilation with intensivists.
November 15, 2024 at 2:28 PM
I used to be on Twitter (@ATC_Ventilator) and now join Bluesky; my aim is to discuss topics around the mode Automatic Tube Compensation, weaning, lung physiology and mechanical ventilation with intensivists.
New on medRxiv! “How to minimize mechanical power during mechanical ventilation”
For any given V'min, a tidal volume of twice the anatomic dead space (~4.4 ml/kg in adults) always minimizes elastic mechanical power (the energy needed for lung expansion).
medrxiv.org/content/10.110…
For any given V'min, a tidal volume of twice the anatomic dead space (~4.4 ml/kg in adults) always minimizes elastic mechanical power (the energy needed for lung expansion).
medrxiv.org/content/10.110…
December 5, 2024 at 8:28 PM
New on medRxiv! “How to minimize mechanical power during mechanical ventilation”
For any given V'min, a tidal volume of twice the anatomic dead space (~4.4 ml/kg in adults) always minimizes elastic mechanical power (the energy needed for lung expansion).
medrxiv.org/content/10.110…
For any given V'min, a tidal volume of twice the anatomic dead space (~4.4 ml/kg in adults) always minimizes elastic mechanical power (the energy needed for lung expansion).
medrxiv.org/content/10.110…
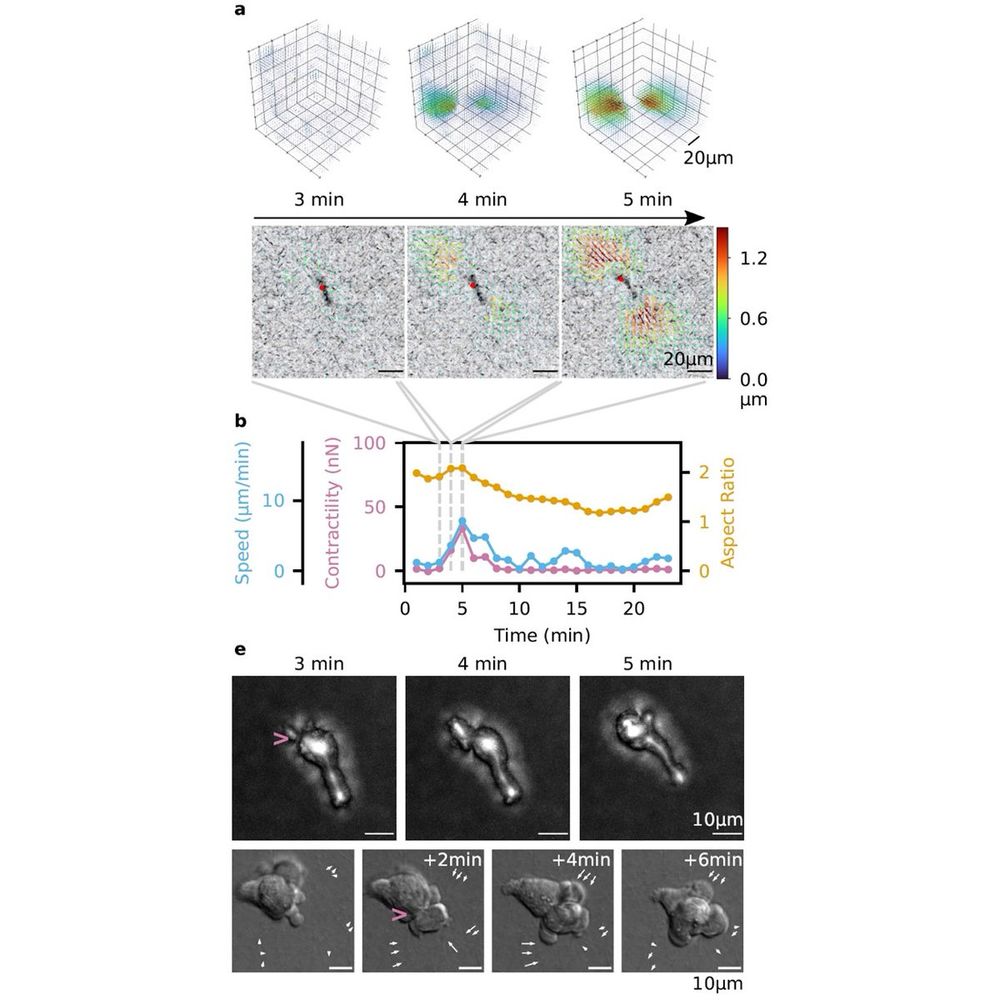
The inflamed lung is full of immune cells, but how do they get there? We found that immune cells can generate large traction forces - comparable to fibroblasts - that help them migrate through narrow pores. Read more in Nature Physics:
rdcu.be/dU9Nj
rdcu.be/dU9Nj
December 5, 2024 at 8:28 PM
The inflamed lung is full of immune cells, but how do they get there? We found that immune cells can generate large traction forces - comparable to fibroblasts - that help them migrate through narrow pores. Read more in Nature Physics:
rdcu.be/dU9Nj
rdcu.be/dU9Nj
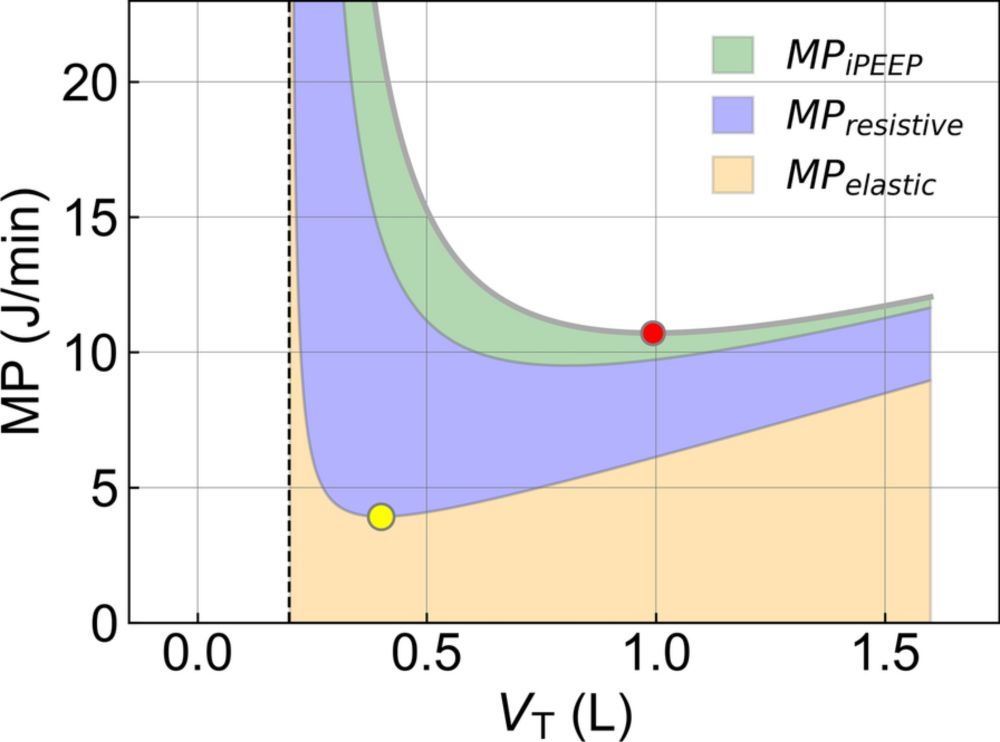
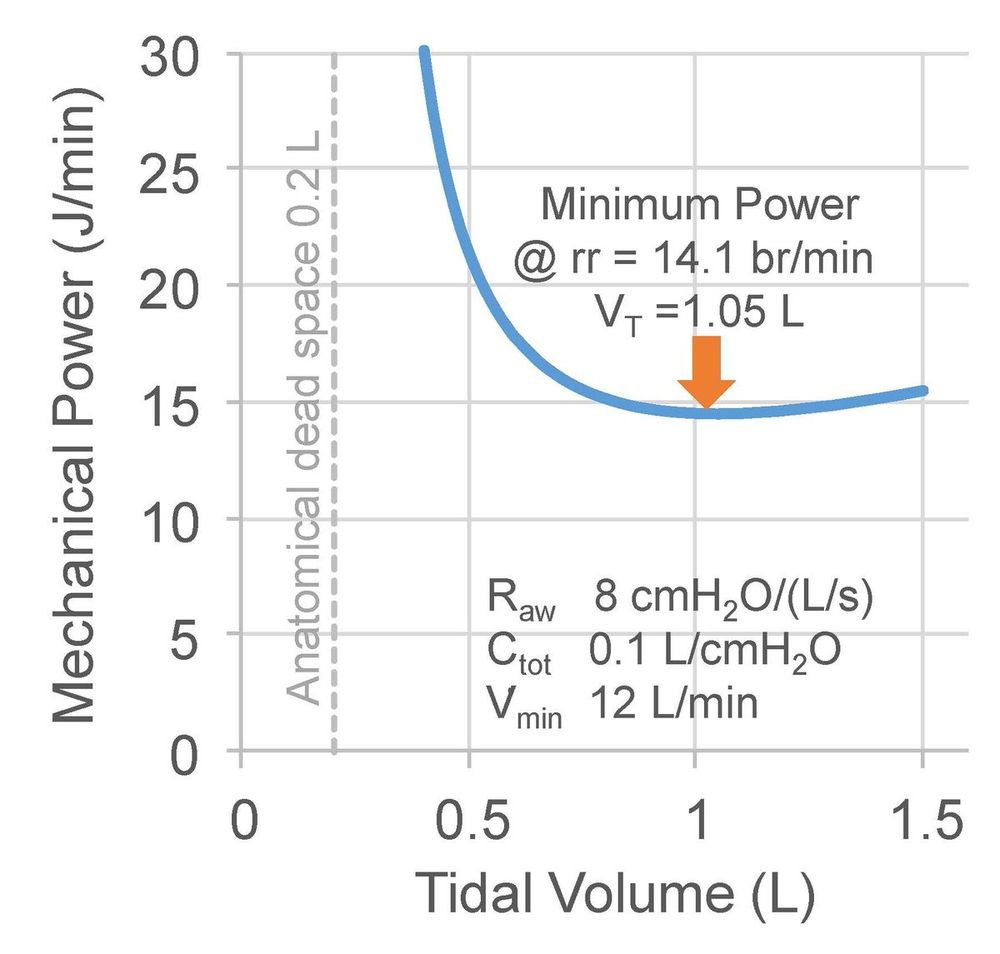
Minimization of Mechanical Power happens at high tidal volumes beyond what is lung-protective. But why? One reason is the resistive work, which decreases at larger tidal volumes. This resistive power is dominated by the resistance of the endotracheal tube.
December 5, 2024 at 8:28 PM
Minimization of Mechanical Power happens at high tidal volumes beyond what is lung-protective. But why? One reason is the resistive work, which decreases at larger tidal volumes. This resistive power is dominated by the resistance of the endotracheal tube.
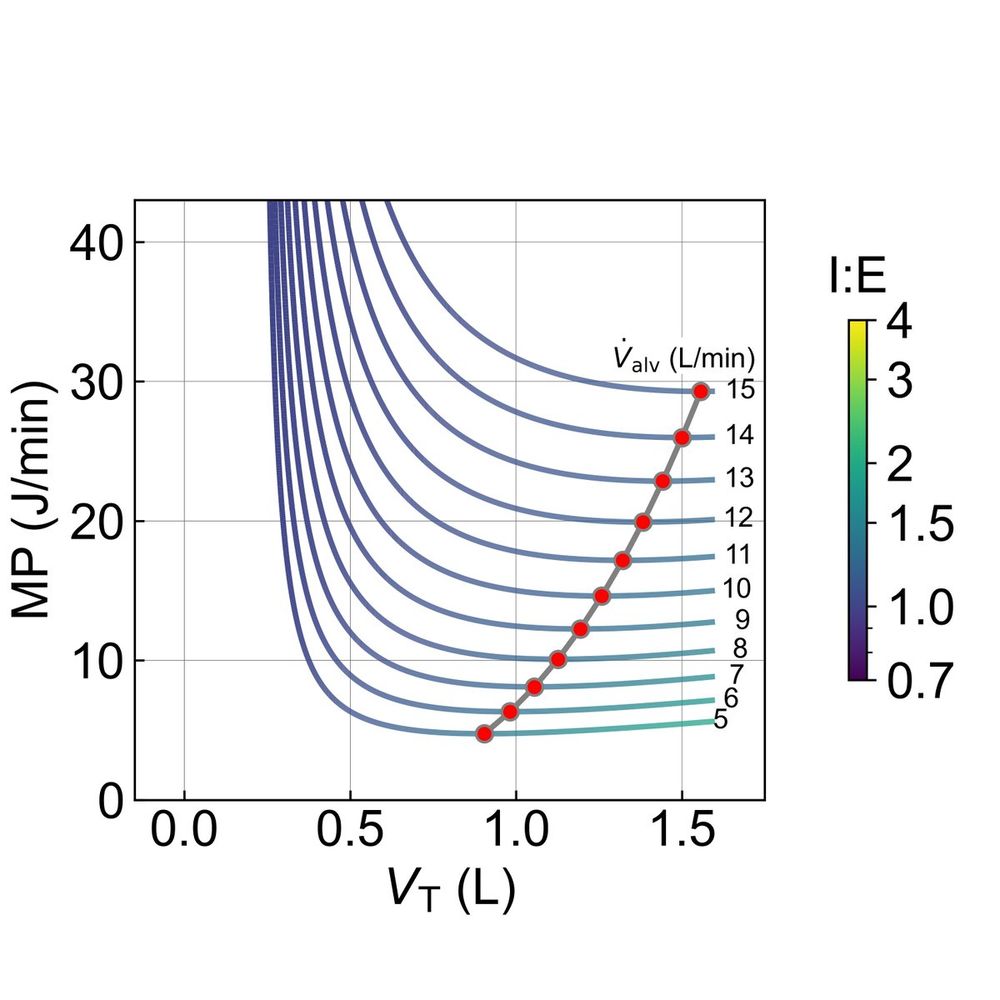
For a given alveolar minute ventilation, which combination of frequency and volume minimizes mechanical power according to the @Gattinon equation? This depends on lung parameters but may result in dangerously high tidal volumes. DO NOT try to minimize the mechanical power.
December 5, 2024 at 8:27 PM
For a given alveolar minute ventilation, which combination of frequency and volume minimizes mechanical power according to the @Gattinon equation? This depends on lung parameters but may result in dangerously high tidal volumes. DO NOT try to minimize the mechanical power.
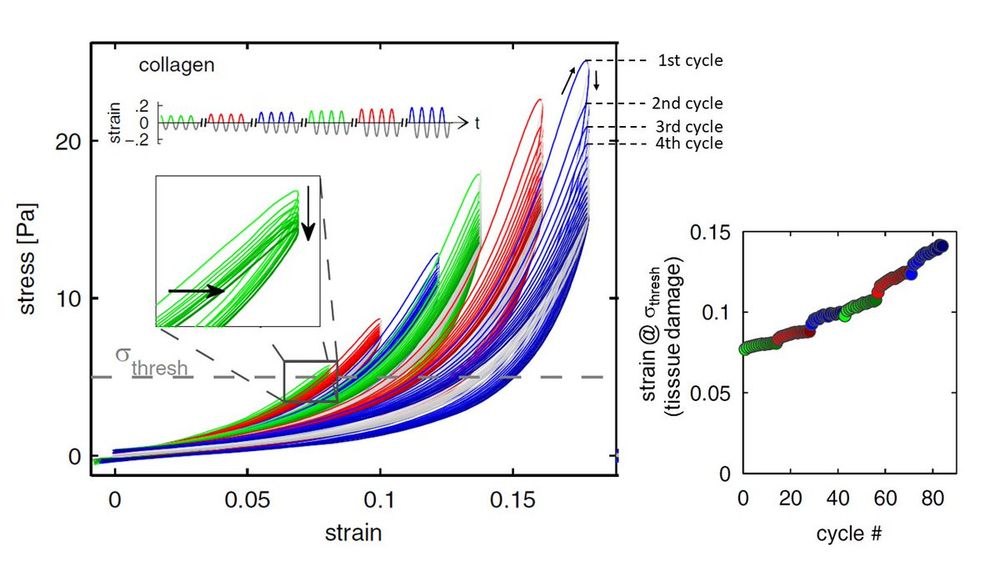
Excessive strain (e.g. due to a large tidal volume) causes tissue damage due to overdistension, but most of the damage occurs already in the first cycle. Subsequent cycles add smaller and smaller increments.@thomasanderson
@gattinon
bio.physik.fau.de/publications/M…
@gattinon
bio.physik.fau.de/publications/M…
December 5, 2024 at 8:27 PM
Excessive strain (e.g. due to a large tidal volume) causes tissue damage due to overdistension, but most of the damage occurs already in the first cycle. Subsequent cycles add smaller and smaller increments.@thomasanderson
@gattinon
bio.physik.fau.de/publications/M…
@gattinon
bio.physik.fau.de/publications/M…
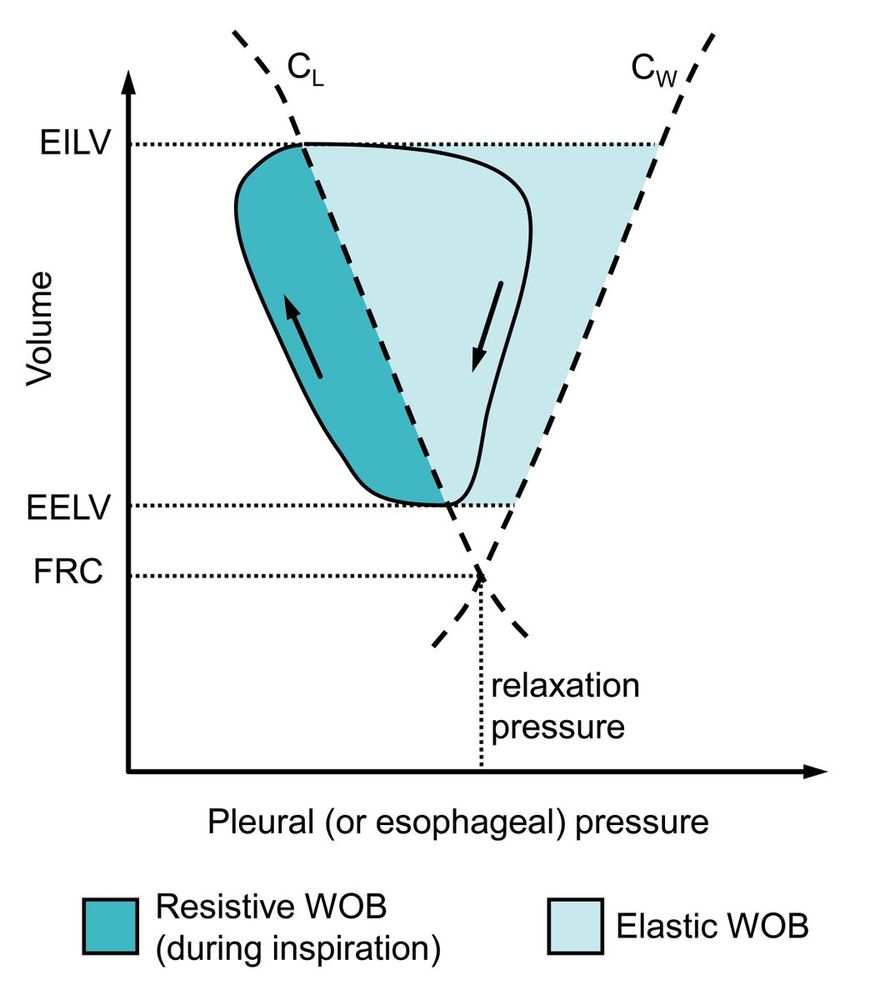
This is how the elastic work of breathing (WOB) is depicted in a Campbell diagram, which was misrepresented in a recent @ERSpublications on ventilatory muscle recruitment during exercise in patients with COPD and interstitial lung disease:
bit.ly/3HVrsuh
bit.ly/3HVrsuh
December 5, 2024 at 8:27 PM
This is how the elastic work of breathing (WOB) is depicted in a Campbell diagram, which was misrepresented in a recent @ERSpublications on ventilatory muscle recruitment during exercise in patients with COPD and interstitial lung disease:
bit.ly/3HVrsuh
bit.ly/3HVrsuh
Great Blue Journal viewpoint on "Mechanical Power and Ventilator-induced Lung Injury: What Does Physics Have to Say?.. physical first principles dictate that purely elastic work delivered during inspiration has no impact on tissue damage."
doi.org/10.1164/rccm.2…
doi.org/10.1164/rccm.2…
Mechanical Power and Ventilator-induced Lung Injury: What Does Physics Have to Say?
Ventilator-induced lung injury (VILI) is a potential threat to anyone receiving supportive mechanical ventilation for acute respiratory failure. Despite decades of research, however, the safest way to ventilate any given patient remains controversial. This makes fertile ground for novel concepts, and one that has arisen recently concerns the idea that a ventilator imparts potentially damaging mechanical energy to the lungs (1, 2). The motivation for this concept is clear: Energy transfer is involved when any structure becomes physically damaged. It may be intuitive, then, that the rate at which energy is delivered to the lungs by a ventilator—namely, mechanical power—should be associated with VILI. Nevertheless, understanding the relationship between mechanical power and VILI requires clarity on the difference between stored versus dissipated energy, regardless of whether ventilation is caused by positive pressure at the airway opening or negative pressure in the pleural space (3).
doi.org
December 5, 2024 at 8:27 PM
Great Blue Journal viewpoint on "Mechanical Power and Ventilator-induced Lung Injury: What Does Physics Have to Say?.. physical first principles dictate that purely elastic work delivered during inspiration has no impact on tissue damage."
doi.org/10.1164/rccm.2…
doi.org/10.1164/rccm.2…
Lumping together PEEP, peak pressure, volume, and what have you into a half-baked formula for mechanical power obfuscates the real issues: stiff lungs, high pressure, regional lung tissue overdistension, and atelectrauma.
December 5, 2024 at 8:27 PM
Lumping together PEEP, peak pressure, volume, and what have you into a half-baked formula for mechanical power obfuscates the real issues: stiff lungs, high pressure, regional lung tissue overdistension, and atelectrauma.
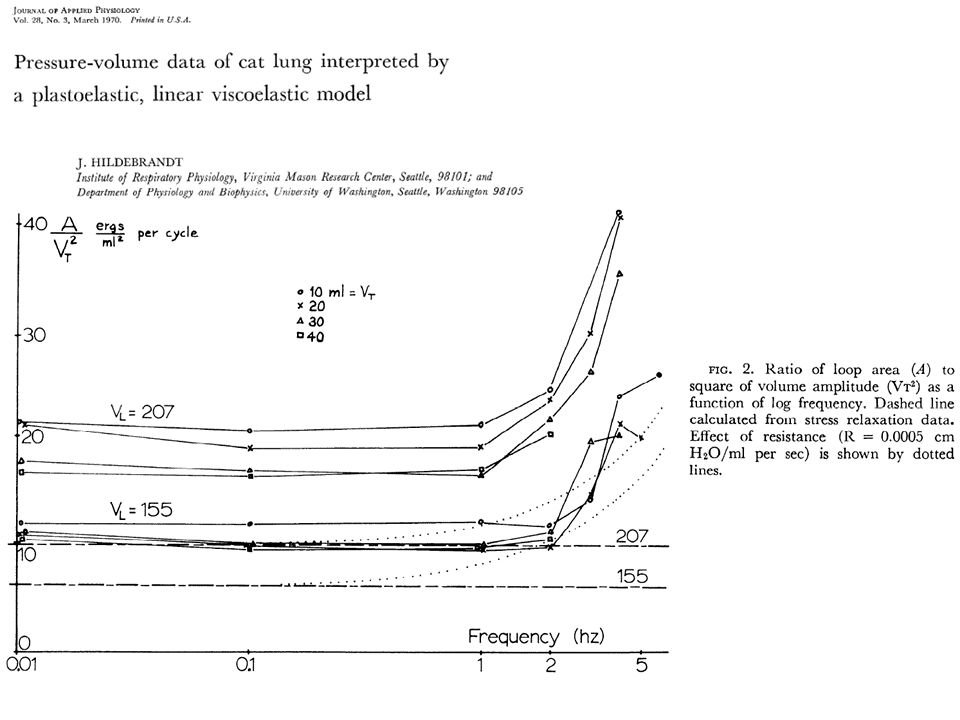
Lung tissue is a weakly frequency-dependent power-law material. This means that the mechanical power dissipated by lung tissue increases only weakly with frequency, and that all(!) simplified equations to estimate the mechanical power during mech. ventilation are deeply flawed.
December 5, 2024 at 8:27 PM
Lung tissue is a weakly frequency-dependent power-law material. This means that the mechanical power dissipated by lung tissue increases only weakly with frequency, and that all(!) simplified equations to estimate the mechanical power during mech. ventilation are deeply flawed.
The dogma that small tidal volumes are lung protective may be wrong for spontaneously breathing ARDS patients with high respiratory drive. Limiting the tidal volume (= flow starvation) leads to negative pressure, which contributes to "patient-induced lung injury".

December 5, 2024 at 8:27 PM
The dogma that small tidal volumes are lung protective may be wrong for spontaneously breathing ARDS patients with high respiratory drive. Limiting the tidal volume (= flow starvation) leads to negative pressure, which contributes to "patient-induced lung injury".
Higher pressure support causes higher tidal volume and more dyssynchrony. Total disaster for PS > 10. Patient’s inspiration = downward hatched; ventilator “support” = upward hatched area. R_aw = 2 mbar/l/s, C_tot = 50 ml/mbar, 7 mm ETT, muscle effort 5 mbar. Simulated data.

December 5, 2024 at 8:27 PM
Higher pressure support causes higher tidal volume and more dyssynchrony. Total disaster for PS > 10. Patient’s inspiration = downward hatched; ventilator “support” = upward hatched area. R_aw = 2 mbar/l/s, C_tot = 50 ml/mbar, 7 mm ETT, muscle effort 5 mbar. Simulated data.
I need your input: I am building a ventilator that can provide near perfect Proportional Assist Ventilation (PAV) and Automatic Tube Compensation (ATC). In addition, I also want the ventilator to provide the essential modes. What are the essential modes? And why? (1/4

December 5, 2024 at 8:27 PM
I need your input: I am building a ventilator that can provide near perfect Proportional Assist Ventilation (PAV) and Automatic Tube Compensation (ATC). In addition, I also want the ventilator to provide the essential modes. What are the essential modes? And why? (1/4
Respirator and anaesthesia ventilator at the German Antarctic Research Station (Neumayer III, Queen Maud Land). Well equipped for emergencies. We have two doctors (surgeons) with us, just in case.



December 5, 2024 at 8:26 PM
Respirator and anaesthesia ventilator at the German Antarctic Research Station (Neumayer III, Queen Maud Land). Well equipped for emergencies. We have two doctors (surgeons) with us, just in case.
I am back in Antarctica doing penguin research. Avian flu has not arrived here yet, but elsewhere in Antarctica, and we are very concerned. Emperor penguins are such magnificent animals and they are already severely threatened by global warming.

December 5, 2024 at 8:26 PM
I am back in Antarctica doing penguin research. Avian flu has not arrived here yet, but elsewhere in Antarctica, and we are very concerned. Emperor penguins are such magnificent animals and they are already severely threatened by global warming.
The resistance of the endotracheal tube is inversely proportional to its radius (or diameter) raised to the fourth (4th !!!) power. This is known as Poiseuille’s law. A 10 % smaller diameter increases the resistance by more than 50%.

December 5, 2024 at 8:26 PM
The resistance of the endotracheal tube is inversely proportional to its radius (or diameter) raised to the fourth (4th !!!) power. This is known as Poiseuille’s law. A 10 % smaller diameter increases the resistance by more than 50%.