


@atc-ventilator.bsky.social
Developed the Automatic Tube Compensation mode (that was my PhD project) in 1993, now Prof. of Physics at Erlangen University (Germany), main research in cellular mechanobiology https://bio.physik.fau.de/
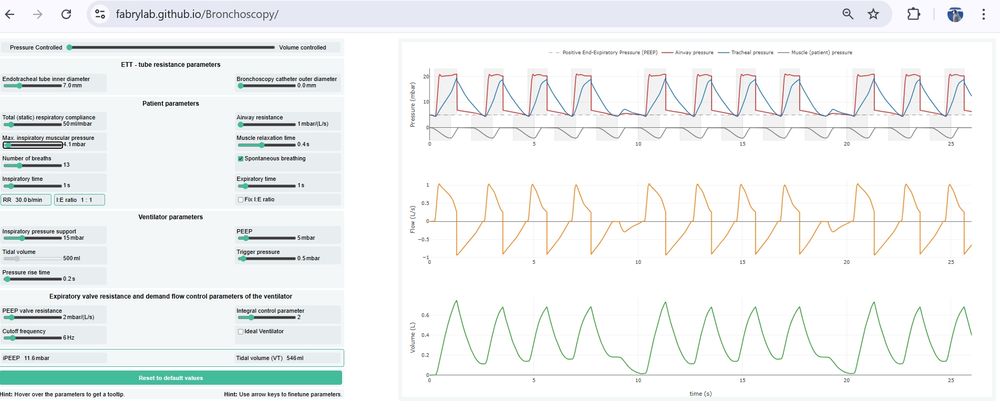
We developed a browser-based tool to predict ventilation impairments such as iPEEP buildup, hypoventilation, and desynchronization due to the tube resistance (also during bronchoscopy). Check it out: fabrylab.github.io/Bronchoscopy/
May 13, 2025 at 8:41 AM
We developed a browser-based tool to predict ventilation impairments such as iPEEP buildup, hypoventilation, and desynchronization due to the tube resistance (also during bronchoscopy). Check it out: fabrylab.github.io/Bronchoscopy/
Yesterday, with the retirement symposium of my academic mentor Jeff Fredberg, the era of respiratory physiology research at the Harvard School of Public Health that began with Jim Whittenberger in 1948 came to an end.

December 15, 2024 at 2:37 PM
Yesterday, with the retirement symposium of my academic mentor Jeff Fredberg, the era of respiratory physiology research at the Harvard School of Public Health that began with Jim Whittenberger in 1948 came to an end.
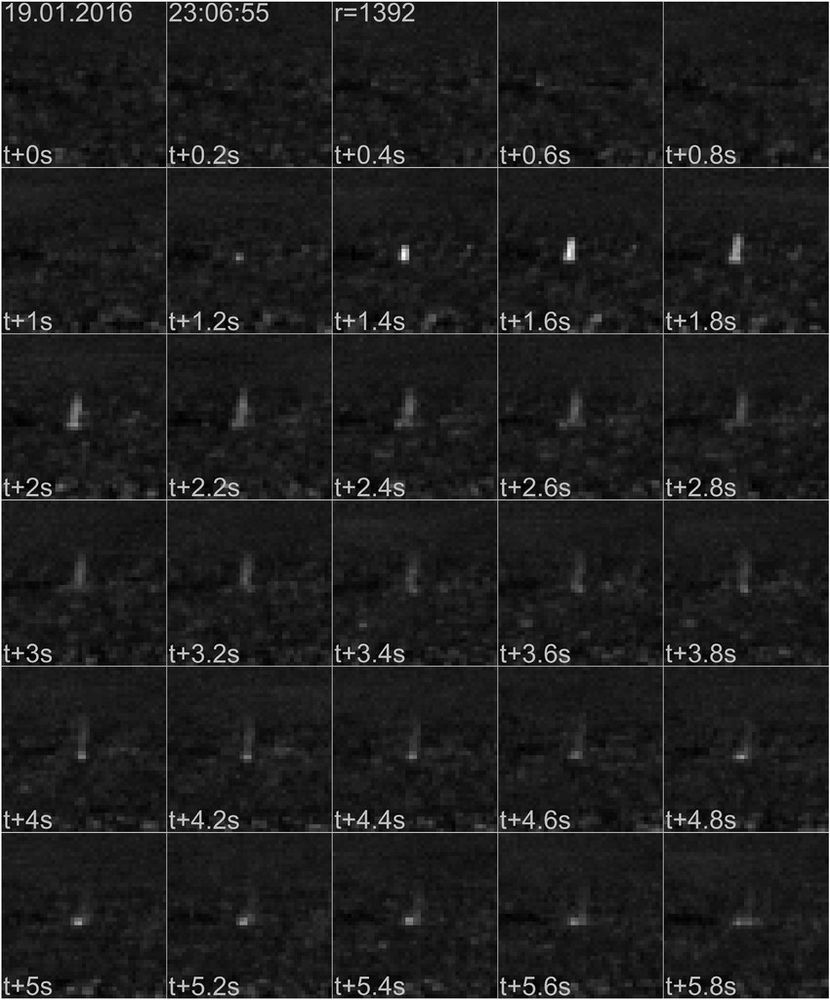
.. and just in case you are wondering what whale research has to do with respiratory physiology - have you ever seen a whale blow? We develop thermal imaging systems that pick up the thermal signature of whale blows to study whale ecology. doi.org/10.1175/JTEC...
December 10, 2024 at 12:29 PM
.. and just in case you are wondering what whale research has to do with respiratory physiology - have you ever seen a whale blow? We develop thermal imaging systems that pick up the thermal signature of whale blows to study whale ecology. doi.org/10.1175/JTEC...
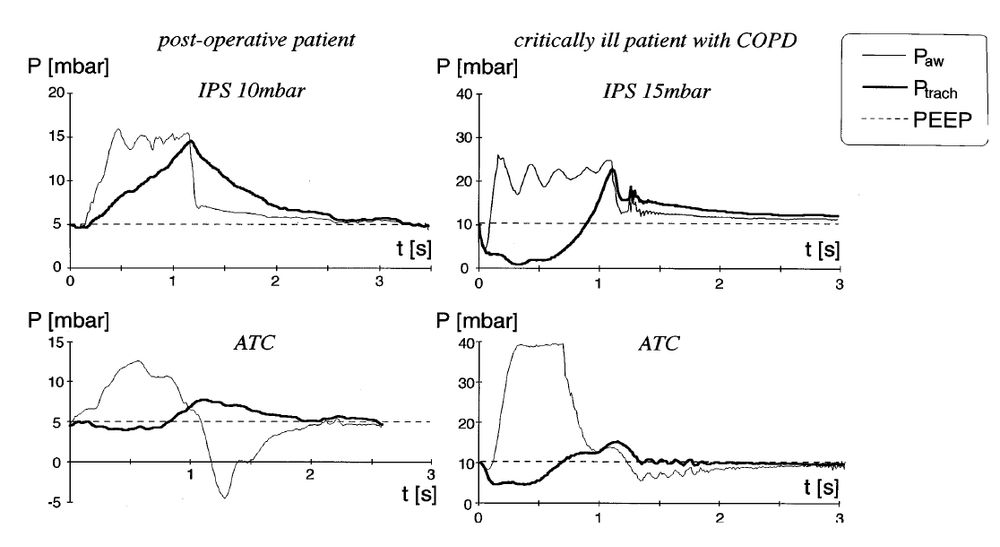
Not sure I understand the question. Perhaps this: A pressure support of 15 mbar is adequate for "normal" patients, but not for those with higher resp. drive (Vmin > 10 L/min). doi.org/10.1007/s001...
December 10, 2024 at 9:08 AM
Not sure I understand the question. Perhaps this: A pressure support of 15 mbar is adequate for "normal" patients, but not for those with higher resp. drive (Vmin > 10 L/min). doi.org/10.1007/s001...
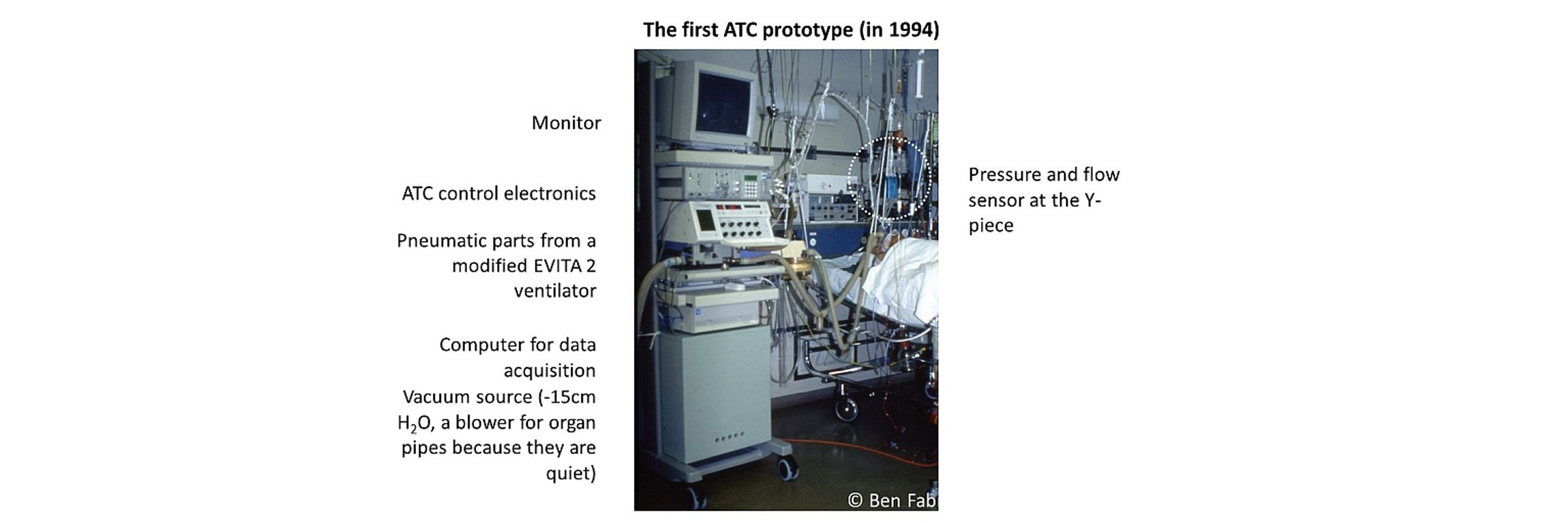
I used to be on Twitter (@ATC_Ventilator) and now join Bluesky; my aim is to discuss topics around the mode Automatic Tube Compensation, weaning, lung physiology and mechanical ventilation with intensivists.
November 15, 2024 at 2:28 PM
I used to be on Twitter (@ATC_Ventilator) and now join Bluesky; my aim is to discuss topics around the mode Automatic Tube Compensation, weaning, lung physiology and mechanical ventilation with intensivists.
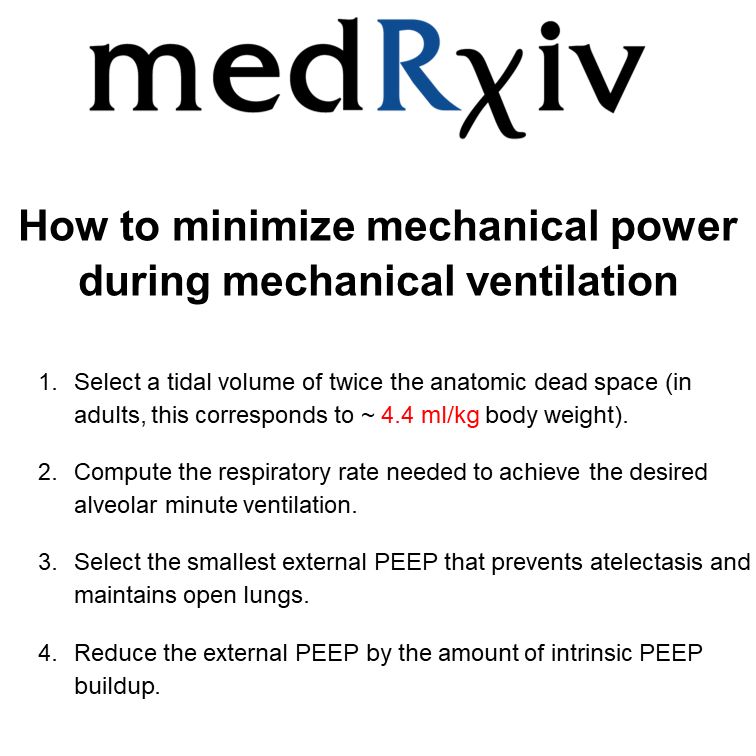
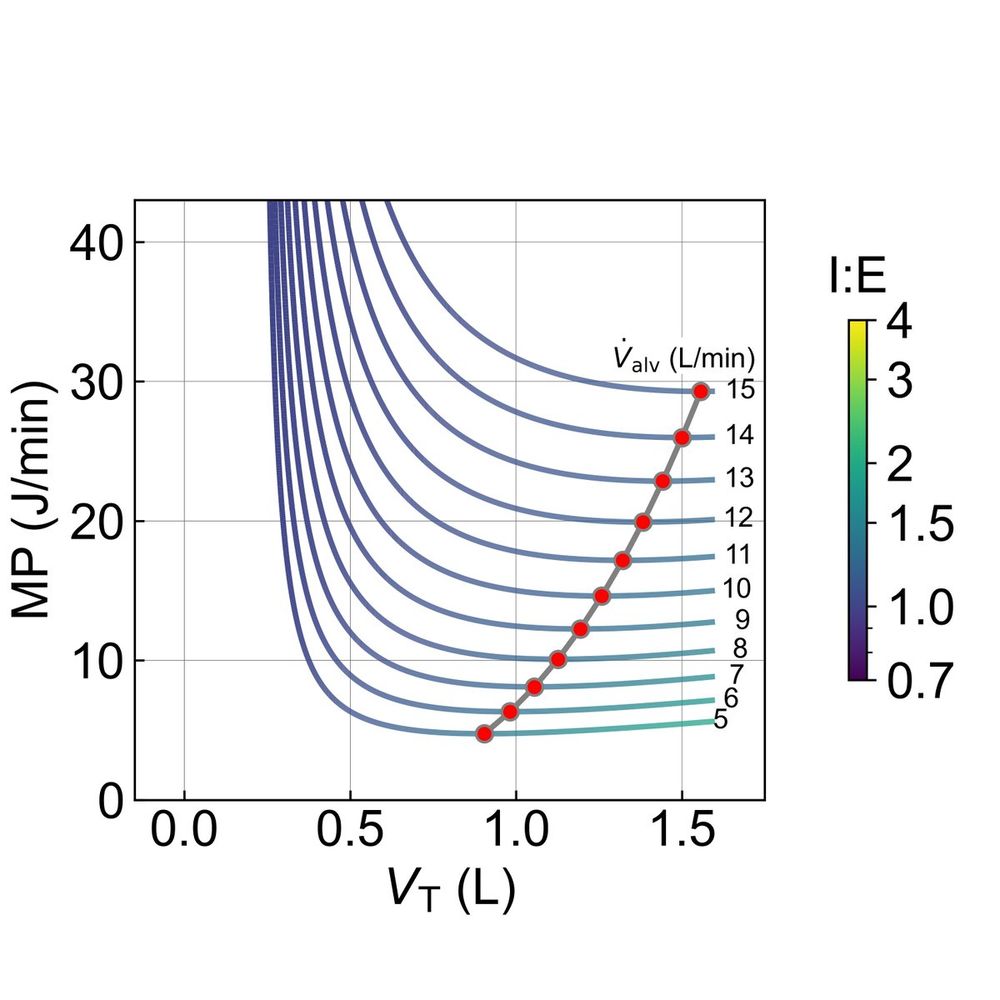
New on medRxiv! “How to minimize mechanical power during mechanical ventilation”
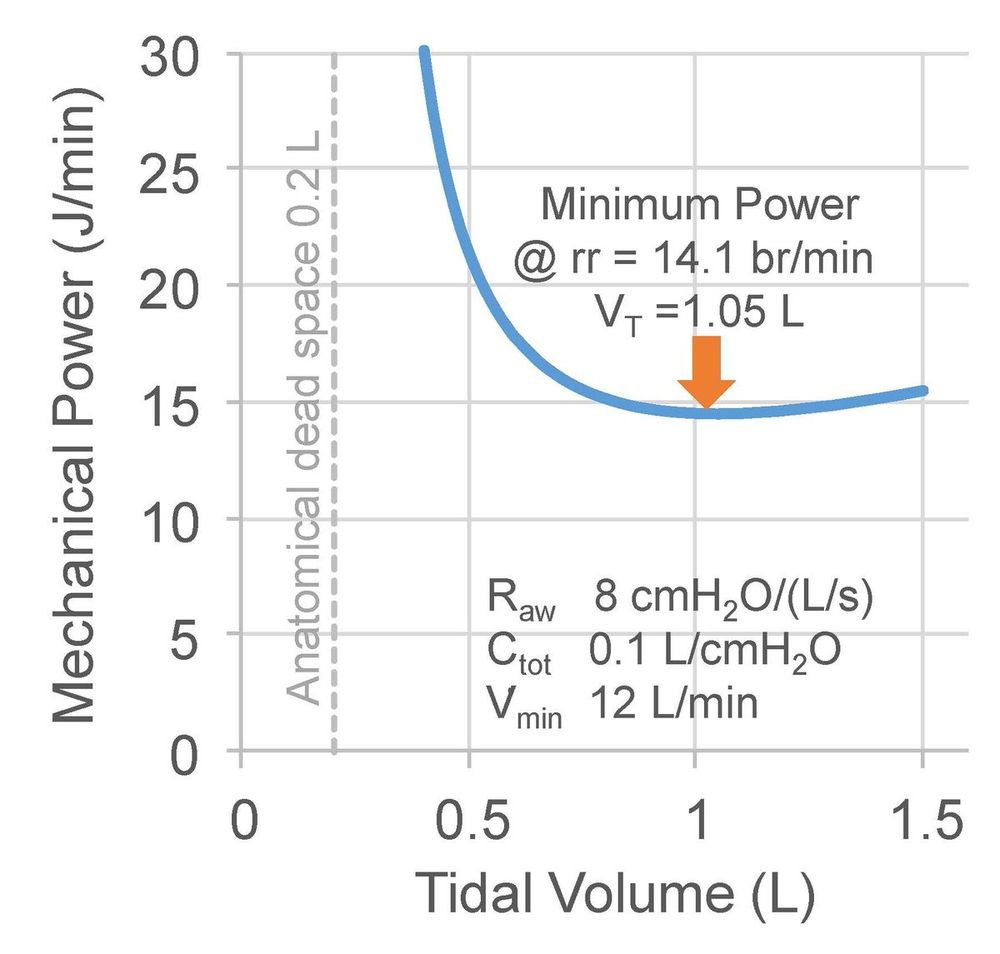
For any given V'min, a tidal volume of twice the anatomic dead space (~4.4 ml/kg in adults) always minimizes elastic mechanical power (the energy needed for lung expansion).
medrxiv.org/content/10.110…
For any given V'min, a tidal volume of twice the anatomic dead space (~4.4 ml/kg in adults) always minimizes elastic mechanical power (the energy needed for lung expansion).
medrxiv.org/content/10.110…
December 5, 2024 at 8:28 PM
New on medRxiv! “How to minimize mechanical power during mechanical ventilation”
For any given V'min, a tidal volume of twice the anatomic dead space (~4.4 ml/kg in adults) always minimizes elastic mechanical power (the energy needed for lung expansion).
medrxiv.org/content/10.110…
For any given V'min, a tidal volume of twice the anatomic dead space (~4.4 ml/kg in adults) always minimizes elastic mechanical power (the energy needed for lung expansion).
medrxiv.org/content/10.110…
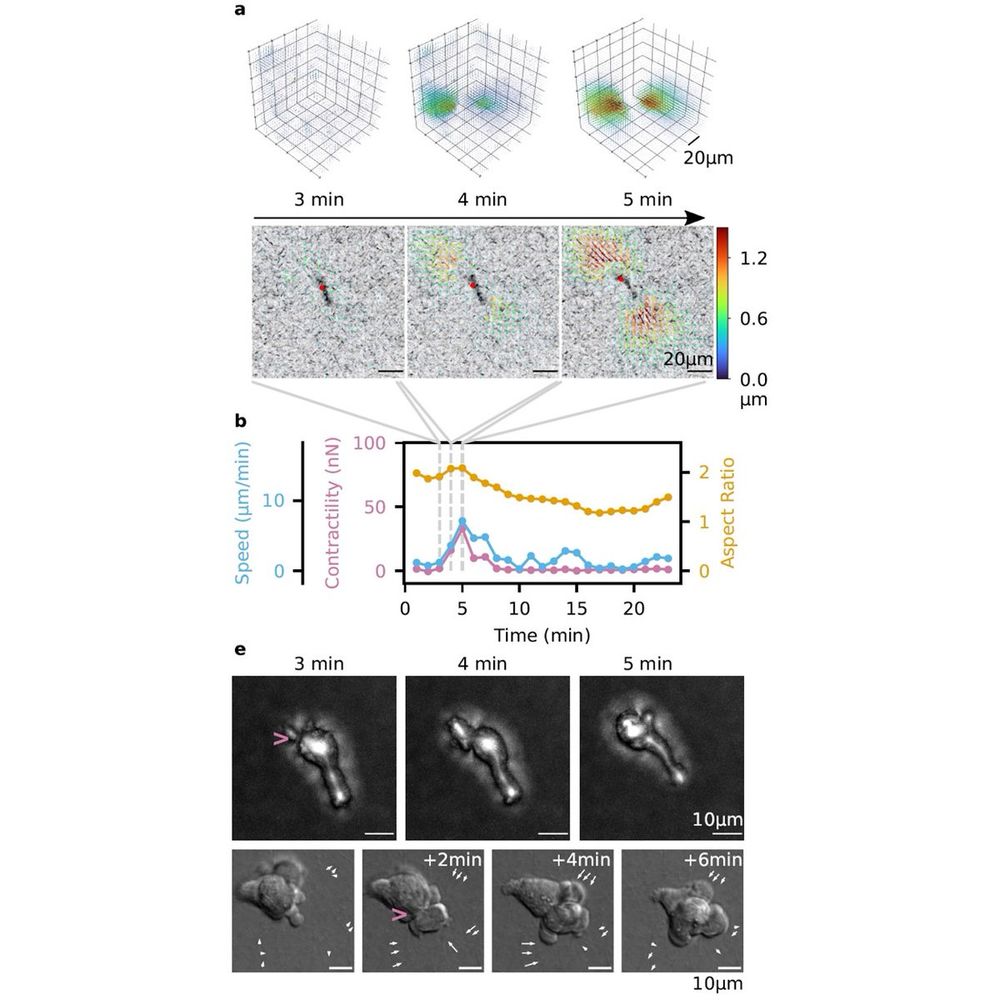
The inflamed lung is full of immune cells, but how do they get there? We found that immune cells can generate large traction forces - comparable to fibroblasts - that help them migrate through narrow pores. Read more in Nature Physics:
rdcu.be/dU9Nj
rdcu.be/dU9Nj
December 5, 2024 at 8:28 PM
The inflamed lung is full of immune cells, but how do they get there? We found that immune cells can generate large traction forces - comparable to fibroblasts - that help them migrate through narrow pores. Read more in Nature Physics:
rdcu.be/dU9Nj
rdcu.be/dU9Nj
Minimization of Mechanical Power happens at high tidal volumes beyond what is lung-protective. But why? One reason is the resistive work, which decreases at larger tidal volumes. This resistive power is dominated by the resistance of the endotracheal tube.
December 5, 2024 at 8:28 PM
Minimization of Mechanical Power happens at high tidal volumes beyond what is lung-protective. But why? One reason is the resistive work, which decreases at larger tidal volumes. This resistive power is dominated by the resistance of the endotracheal tube.
For a given alveolar minute ventilation, which combination of frequency and volume minimizes mechanical power according to the @Gattinon equation? This depends on lung parameters but may result in dangerously high tidal volumes. DO NOT try to minimize the mechanical power.
December 5, 2024 at 8:27 PM
For a given alveolar minute ventilation, which combination of frequency and volume minimizes mechanical power according to the @Gattinon equation? This depends on lung parameters but may result in dangerously high tidal volumes. DO NOT try to minimize the mechanical power.
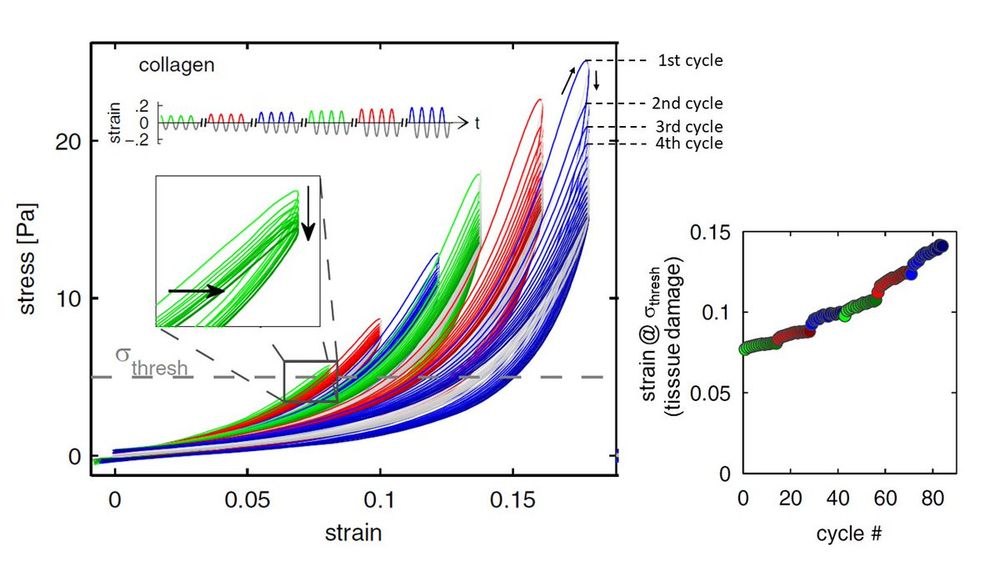
Excessive strain (e.g. due to a large tidal volume) causes tissue damage due to overdistension, but most of the damage occurs already in the first cycle. Subsequent cycles add smaller and smaller increments.@thomasanderson
@gattinon
bio.physik.fau.de/publications/M…
@gattinon
bio.physik.fau.de/publications/M…
December 5, 2024 at 8:27 PM
Excessive strain (e.g. due to a large tidal volume) causes tissue damage due to overdistension, but most of the damage occurs already in the first cycle. Subsequent cycles add smaller and smaller increments.@thomasanderson
@gattinon
bio.physik.fau.de/publications/M…
@gattinon
bio.physik.fau.de/publications/M…
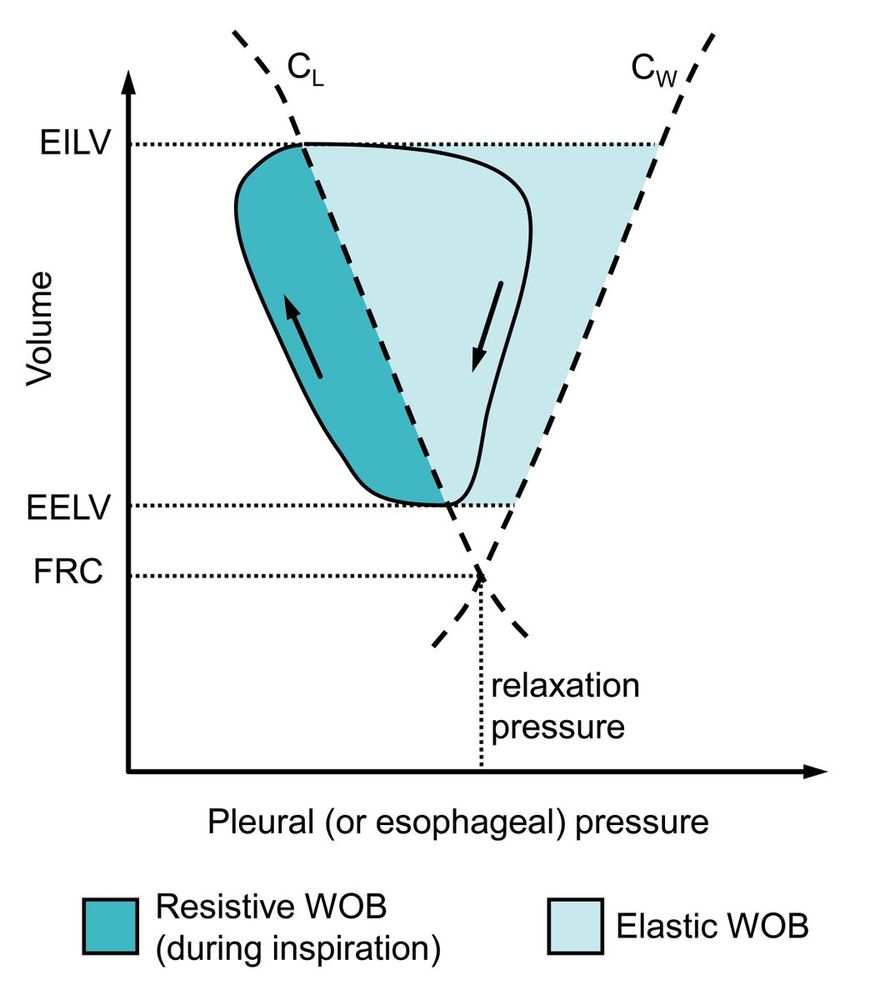
This is how the elastic work of breathing (WOB) is depicted in a Campbell diagram, which was misrepresented in a recent @ERSpublications on ventilatory muscle recruitment during exercise in patients with COPD and interstitial lung disease:
bit.ly/3HVrsuh
bit.ly/3HVrsuh
December 5, 2024 at 8:27 PM
This is how the elastic work of breathing (WOB) is depicted in a Campbell diagram, which was misrepresented in a recent @ERSpublications on ventilatory muscle recruitment during exercise in patients with COPD and interstitial lung disease:
bit.ly/3HVrsuh
bit.ly/3HVrsuh
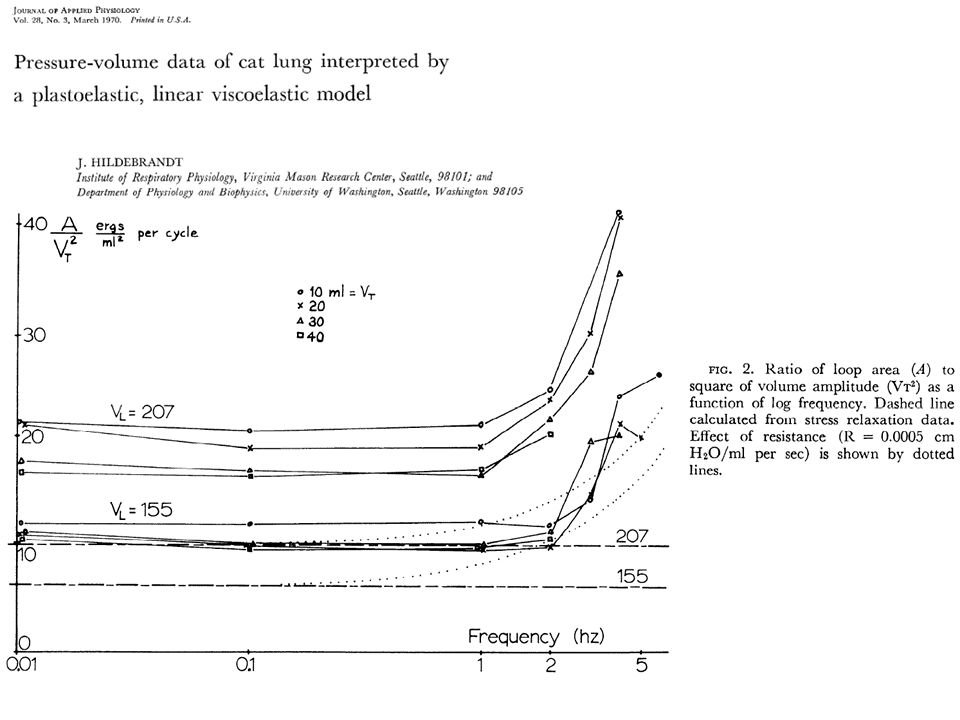
Lung tissue is a weakly frequency-dependent power-law material. This means that the mechanical power dissipated by lung tissue increases only weakly with frequency, and that all(!) simplified equations to estimate the mechanical power during mech. ventilation are deeply flawed.
December 5, 2024 at 8:27 PM
Lung tissue is a weakly frequency-dependent power-law material. This means that the mechanical power dissipated by lung tissue increases only weakly with frequency, and that all(!) simplified equations to estimate the mechanical power during mech. ventilation are deeply flawed.
The dogma that small tidal volumes are lung protective may be wrong for spontaneously breathing ARDS patients with high respiratory drive. Limiting the tidal volume (= flow starvation) leads to negative pressure, which contributes to "patient-induced lung injury".

December 5, 2024 at 8:27 PM
The dogma that small tidal volumes are lung protective may be wrong for spontaneously breathing ARDS patients with high respiratory drive. Limiting the tidal volume (= flow starvation) leads to negative pressure, which contributes to "patient-induced lung injury".
Higher pressure support causes higher tidal volume and more dyssynchrony. Total disaster for PS > 10. Patient’s inspiration = downward hatched; ventilator “support” = upward hatched area. R_aw = 2 mbar/l/s, C_tot = 50 ml/mbar, 7 mm ETT, muscle effort 5 mbar. Simulated data.

December 5, 2024 at 8:27 PM
Higher pressure support causes higher tidal volume and more dyssynchrony. Total disaster for PS > 10. Patient’s inspiration = downward hatched; ventilator “support” = upward hatched area. R_aw = 2 mbar/l/s, C_tot = 50 ml/mbar, 7 mm ETT, muscle effort 5 mbar. Simulated data.
I need your input: I am building a ventilator that can provide near perfect Proportional Assist Ventilation (PAV) and Automatic Tube Compensation (ATC). In addition, I also want the ventilator to provide the essential modes. What are the essential modes? And why? (1/4

December 5, 2024 at 8:27 PM
I need your input: I am building a ventilator that can provide near perfect Proportional Assist Ventilation (PAV) and Automatic Tube Compensation (ATC). In addition, I also want the ventilator to provide the essential modes. What are the essential modes? And why? (1/4
Respirator and anaesthesia ventilator at the German Antarctic Research Station (Neumayer III, Queen Maud Land). Well equipped for emergencies. We have two doctors (surgeons) with us, just in case.



December 5, 2024 at 8:26 PM
Respirator and anaesthesia ventilator at the German Antarctic Research Station (Neumayer III, Queen Maud Land). Well equipped for emergencies. We have two doctors (surgeons) with us, just in case.
I am back in Antarctica doing penguin research. Avian flu has not arrived here yet, but elsewhere in Antarctica, and we are very concerned. Emperor penguins are such magnificent animals and they are already severely threatened by global warming.

December 5, 2024 at 8:26 PM
I am back in Antarctica doing penguin research. Avian flu has not arrived here yet, but elsewhere in Antarctica, and we are very concerned. Emperor penguins are such magnificent animals and they are already severely threatened by global warming.
The resistance of the endotracheal tube is inversely proportional to its radius (or diameter) raised to the fourth (4th !!!) power. This is known as Poiseuille’s law. A 10 % smaller diameter increases the resistance by more than 50%.

December 5, 2024 at 8:26 PM
The resistance of the endotracheal tube is inversely proportional to its radius (or diameter) raised to the fourth (4th !!!) power. This is known as Poiseuille’s law. A 10 % smaller diameter increases the resistance by more than 50%.
Thanks to the 14 participants for their votes. ATC or TRC is used more often than I thought. It's not used at our university teaching hospital (Erlangen, Germany). They are so understaffed that ATC is too much trouble, too "experimental". I will write about other reasons later.

December 5, 2024 at 8:26 PM
Thanks to the 14 participants for their votes. ATC or TRC is used more often than I thought. It's not used at our university teaching hospital (Erlangen, Germany). They are so understaffed that ATC is too much trouble, too "experimental". I will write about other reasons later.
Thanks to all who participated. To my knowledge, there is no conclusive study that says who is right or wrong. My own guess is around 10% reduction in mortality - that's huge.

December 5, 2024 at 8:26 PM
Thanks to all who participated. To my knowledge, there is no conclusive study that says who is right or wrong. My own guess is around 10% reduction in mortality - that's huge.
The term “patient self-inflicted lung injury” is an insult to patients. The injury is inflicted by ventilators delivering insufficient support, causing negative alveolar pressure during strong inspiratory efforts. This is preventable with proper tube compensation.

December 5, 2024 at 8:26 PM
The term “patient self-inflicted lung injury” is an insult to patients. The injury is inflicted by ventilators delivering insufficient support, causing negative alveolar pressure during strong inspiratory efforts. This is preventable with proper tube compensation.
What kills lung cells: excessive strain (volume) or stress (pressure)? It’s strain! For the same stress, stiffer cells deform less and survive much better. Bottom line: Avoid volume-controlled ventilation, use pressure-controlled modes instead!
doi.org/10.1088/1758-5…
doi.org/10.1088/1758-5…

December 5, 2024 at 8:26 PM
What kills lung cells: excessive strain (volume) or stress (pressure)? It’s strain! For the same stress, stiffer cells deform less and survive much better. Bottom line: Avoid volume-controlled ventilation, use pressure-controlled modes instead!
doi.org/10.1088/1758-5…
doi.org/10.1088/1758-5…
I tried to compile Chatburn’s taxonomy of ventilatory modes in a simple diagram. I find this taxonomy somewhat unintuitive (e.g. PC-CSVr is the mode ATC) and ambiguous (PAV is also PC-CSVr). And don’t get me started on “optimal” or “intelligent”. But I have no better idea.

December 5, 2024 at 8:26 PM
I tried to compile Chatburn’s taxonomy of ventilatory modes in a simple diagram. I find this taxonomy somewhat unintuitive (e.g. PC-CSVr is the mode ATC) and ambiguous (PAV is also PC-CSVr). And don’t get me started on “optimal” or “intelligent”. But I have no better idea.
Proportional Assist Ventilation (PAV) and Automatic Tube Compensation (ATC) are not for the faint-hearted, quite literally. Low cardiac output causes transport delays between the lungs and the chemoreceptors, which can lead to periodic (Cheyne-Stokes) breathing.

December 5, 2024 at 8:26 PM
Proportional Assist Ventilation (PAV) and Automatic Tube Compensation (ATC) are not for the faint-hearted, quite literally. Low cardiac output causes transport delays between the lungs and the chemoreceptors, which can lead to periodic (Cheyne-Stokes) breathing.
Work of Breathing (WOB) is an elusive concept. I have translated WOB for normal, quiet breathing into the equivalent of a weight on your chest that you have to lift (by 1 cm) with every breath. During a T-piece trial, an 8 mm ETT packs an extra 2.4 kg on your chest.

December 5, 2024 at 8:26 PM
Work of Breathing (WOB) is an elusive concept. I have translated WOB for normal, quiet breathing into the equivalent of a weight on your chest that you have to lift (by 1 cm) with every breath. During a T-piece trial, an 8 mm ETT packs an extra 2.4 kg on your chest.