


@atc-ventilator.bsky.social
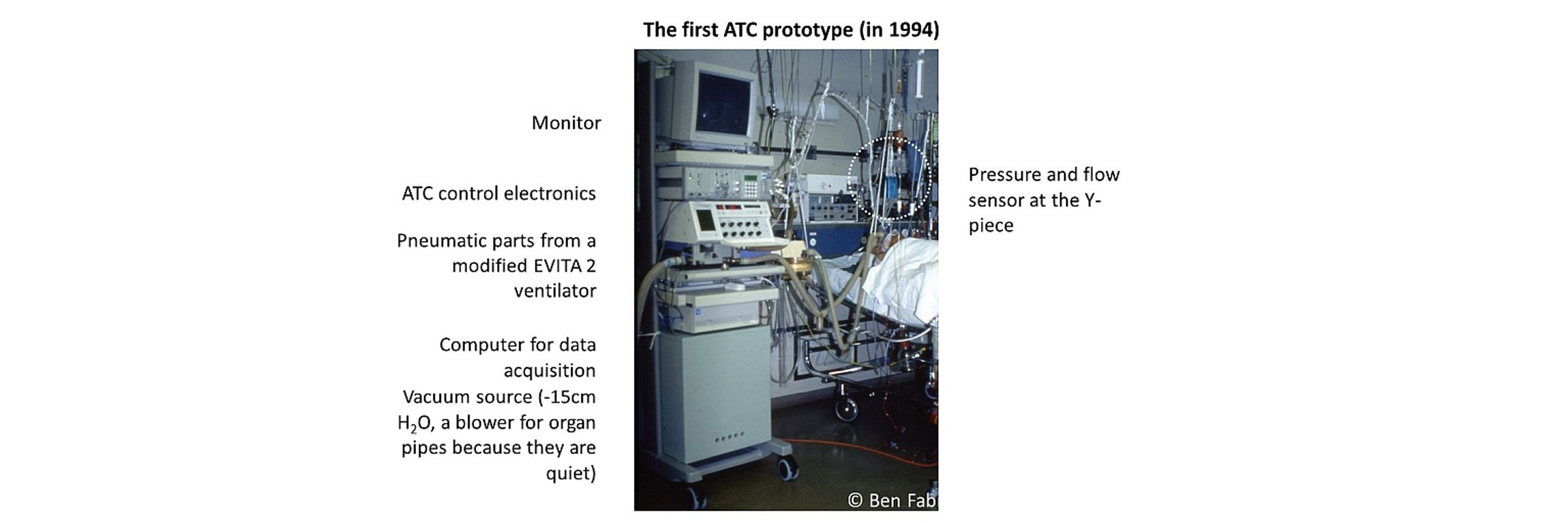
Developed the Automatic Tube Compensation mode (that was my PhD project) in 1993, now Prof. of Physics at Erlangen University (Germany), main research in cellular mechanobiology https://bio.physik.fau.de/
Thank you for your kind words! I think it's a great teaching tool, but realistically, I don't see it being integrated into routine clinical practice, even though patients would benefit from it.
September 2, 2025 at 11:37 AM
Thank you for your kind words! I think it's a great teaching tool, but realistically, I don't see it being integrated into routine clinical practice, even though patients would benefit from it.
Drop me a line if you are interested in this new technology. Also, if you a manufacturer of ventilators, I would love to test one of your ventilators in my lab, if you are willing to loan me one for one or two weeks.
January 15, 2025 at 6:08 PM
Drop me a line if you are interested in this new technology. Also, if you a manufacturer of ventilators, I would love to test one of your ventilators in my lab, if you are willing to loan me one for one or two weeks.
Commercial ventilators often (perhaps all of them?) suffer from sluggish demand-flow delivery and cannot exploit the full potential of ATC. I have therefore developed a new ventilator featuring a fast and precise demand flow controller to deliver proper ATC.
January 15, 2025 at 6:08 PM
Commercial ventilators often (perhaps all of them?) suffer from sluggish demand-flow delivery and cannot exploit the full potential of ATC. I have therefore developed a new ventilator featuring a fast and precise demand flow controller to deliver proper ATC.
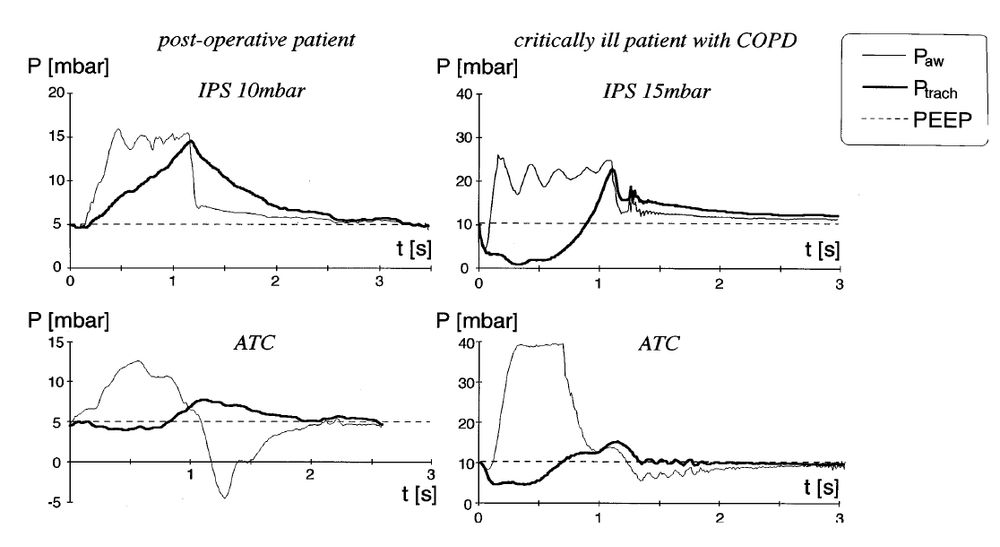
Unfortunately, current pressure support modes cannot deal with weak patients with rapid shallow breathing, or with large inspiratory efforts. The solution to this problem is proper Automatic Tube Compensation (ATC), if needed in combination with proportional assist ventilation (PAV).
January 15, 2025 at 6:08 PM
Unfortunately, current pressure support modes cannot deal with weak patients with rapid shallow breathing, or with large inspiratory efforts. The solution to this problem is proper Automatic Tube Compensation (ATC), if needed in combination with proportional assist ventilation (PAV).
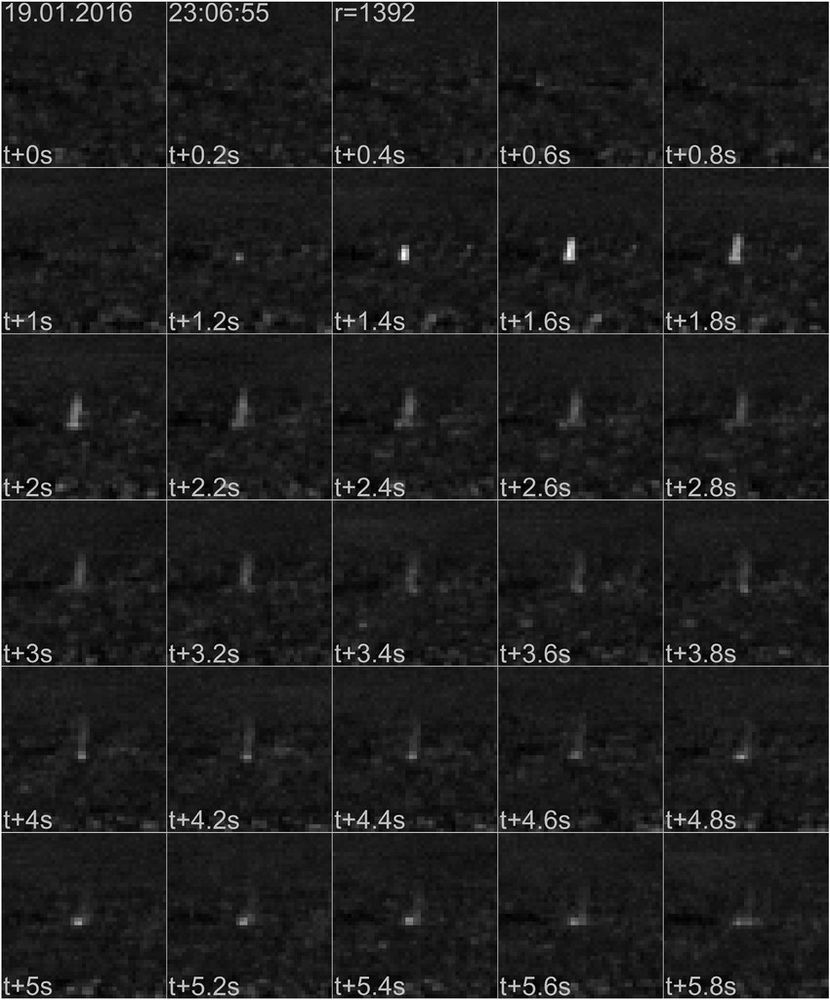
.. and just in case you are wondering what whale research has to do with respiratory physiology - have you ever seen a whale blow? We develop thermal imaging systems that pick up the thermal signature of whale blows to study whale ecology. doi.org/10.1175/JTEC...
December 10, 2024 at 12:29 PM
.. and just in case you are wondering what whale research has to do with respiratory physiology - have you ever seen a whale blow? We develop thermal imaging systems that pick up the thermal signature of whale blows to study whale ecology. doi.org/10.1175/JTEC...
Not sure I understand the question. Perhaps this: A pressure support of 15 mbar is adequate for "normal" patients, but not for those with higher resp. drive (Vmin > 10 L/min). doi.org/10.1007/s001...
December 10, 2024 at 9:08 AM
Not sure I understand the question. Perhaps this: A pressure support of 15 mbar is adequate for "normal" patients, but not for those with higher resp. drive (Vmin > 10 L/min). doi.org/10.1007/s001...
I visited a cardiac ICU almost every day for 5 years and never saw a case of VILI. Of course, you don't want to overinflate the healthy lungs of cardiac patients, but that's mainly for hemodynamic reasons.
December 10, 2024 at 9:02 AM
I visited a cardiac ICU almost every day for 5 years and never saw a case of VILI. Of course, you don't want to overinflate the healthy lungs of cardiac patients, but that's mainly for hemodynamic reasons.
A Python script for the numerical power minimization can be downloaded from github.com/fabrylab/MP_...
GitHub - fabrylab/MP_ventilation: script to compute the ventilator parameters (VT, rr, I:E ratio) that minimize mechanical power for a given alveolar minute ventilation
script to compute the ventilator parameters (VT, rr, I:E ratio) that minimize mechanical power for a given alveolar minute ventilation - fabrylab/MP_ventilation
github.com
December 9, 2024 at 1:41 PM
A Python script for the numerical power minimization can be downloaded from github.com/fabrylab/MP_...
Paw is irrelevant as Ptrach will still remain at PEEP at all times. The patient can freely breathe as if extubated, and is free to choose a small or large tidal volume, like you and me.
December 8, 2024 at 2:55 PM
Paw is irrelevant as Ptrach will still remain at PEEP at all times. The patient can freely breathe as if extubated, and is free to choose a small or large tidal volume, like you and me.
Yes, during a vigorous inspiratory effort, Paw can rise to >35 mbar above PEEP, but that does not cause VILI, rather, it prevents Ptrach and Palv to become negative and hence prevents PSILI.
December 8, 2024 at 1:45 PM
Yes, during a vigorous inspiratory effort, Paw can rise to >35 mbar above PEEP, but that does not cause VILI, rather, it prevents Ptrach and Palv to become negative and hence prevents PSILI.
You mean you are afraid that Paw drops below PEEP during expiration? Don't be. Ptrach will still remain at around PEEP. And also consider that proper ATC, unlike CPAP or PSV, prevents Ptrach to become negative during inspiration.
December 8, 2024 at 12:59 PM
You mean you are afraid that Paw drops below PEEP during expiration? Don't be. Ptrach will still remain at around PEEP. And also consider that proper ATC, unlike CPAP or PSV, prevents Ptrach to become negative during inspiration.
Could not agree more.
December 7, 2024 at 7:45 AM
Could not agree more.