Posts
Media
Videos
Starter Packs



Brad Spellberg
@bradspellberg.bsky.social
· Aug 14

Brad Spellberg
@bradspellberg.bsky.social
· Aug 14

Brad Spellberg
@bradspellberg.bsky.social
· Aug 12
Brad Spellberg
@bradspellberg.bsky.social
· Aug 12
Brad Spellberg
@bradspellberg.bsky.social
· Aug 12
Brad Spellberg
@bradspellberg.bsky.social
· Aug 12
Brad Spellberg
@bradspellberg.bsky.social
· Aug 12



Reposted by Brad Spellberg
Reposted by Brad Spellberg

Brad Spellberg
@bradspellberg.bsky.social
· Jul 21
Brad Spellberg
@bradspellberg.bsky.social
· Jul 21

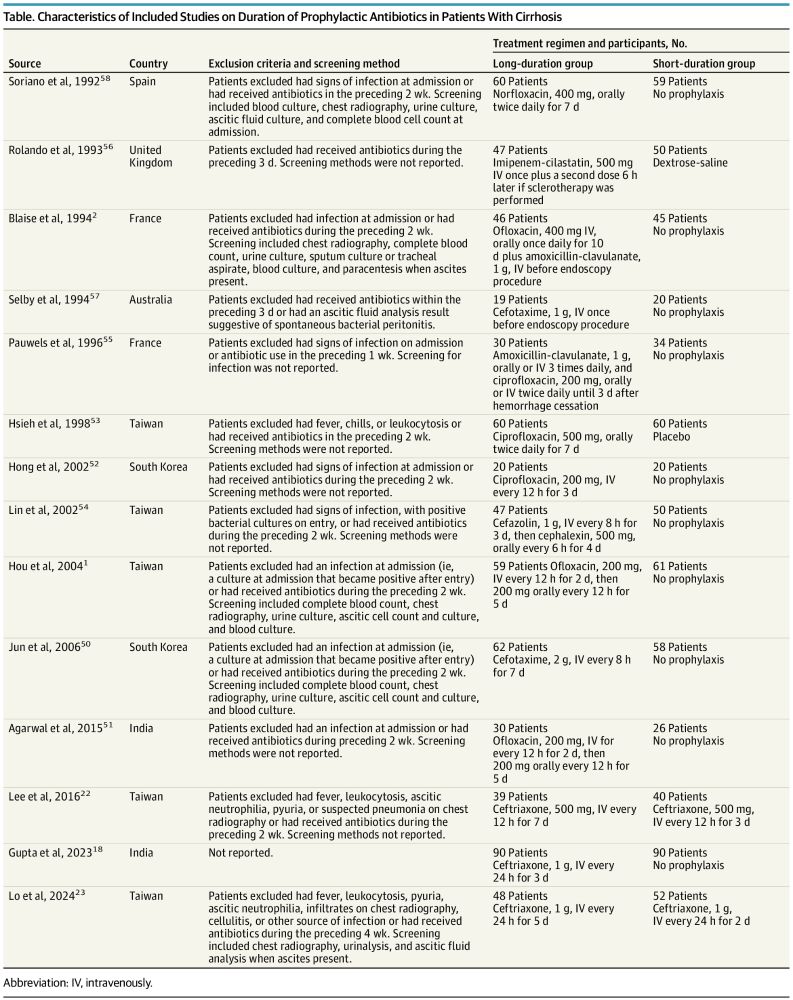
Longer-Duration Antimicrobial Therapy Does Not Prevent Treatment Failure in High-Risk Patients with Complicated Intra-Abdominal Infections - PubMed
We were able to identify patients at high risk for treatment failure in the STOP-IT trial. Such patients did not benefit from a longer course of antibiotic administration. Further study is needed to d...
pubmed.ncbi.nlm.nih.gov
Brad Spellberg
@bradspellberg.bsky.social
· Jul 10


