
Kyle Walding
@tbrnaughttb.bsky.social
5.9K followers
340 following
280 posts
TB doc, Manhattan TB consultant @ NYC Dept of Health
NYU Clinical Asst Professor of ID @ Bellevue Hospital
Loyola Med/Peds & Stanford ID
❤️: TB, ID, med ed, public health, health equity, immigrant safety/rights
Views = mine = great, & ≠ my employers' | 🏳️🌈
Posts
Media
Videos
Starter Packs

Kyle Walding
@tbrnaughttb.bsky.social
· Sep 2
Reposted by Kyle Walding


Reposted by Kyle Walding

Gabriele Pollara
@gpollara.bsky.social
· Jul 18
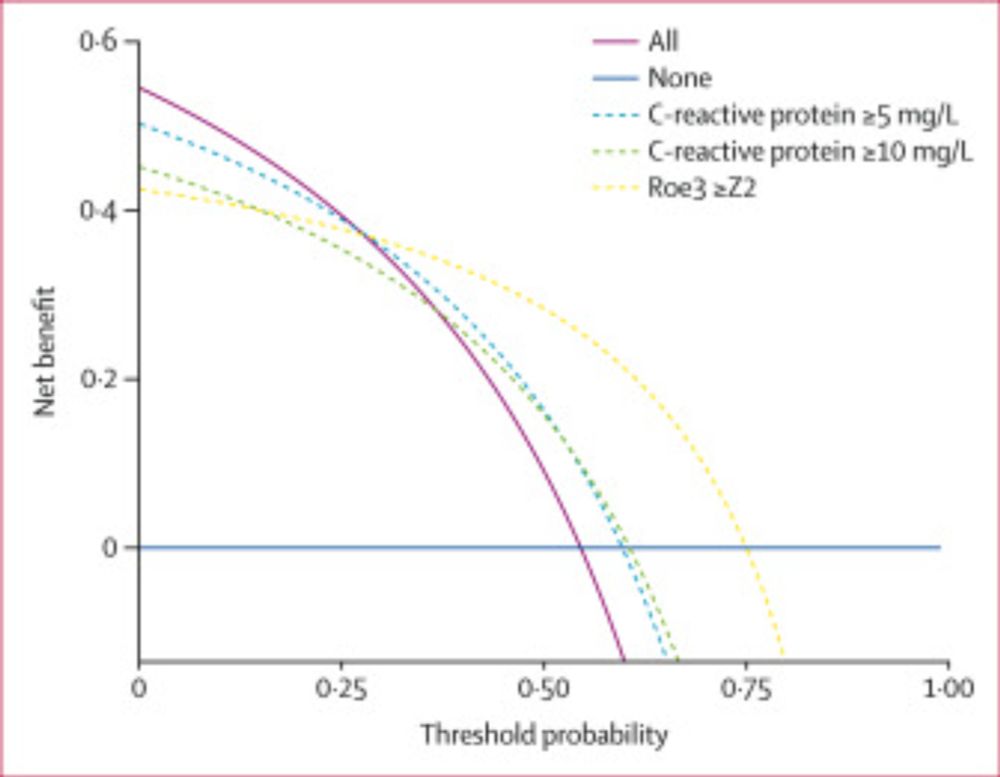
Blood RNA biomarkers and C-reactive protein for triage of adult patients with tuberculosis lymphadenitis and pericarditis in South Africa: a single-centre, prospective, observational, diagnostic accur...
Our results suggest RNA biomarkers show better accuracy and clinical utility than
C-reactive protein to trigger confirmatory tuberculosis testing in patients with tuberculosis
lymphadenitis and tuberc...
www.thelancet.com
Kyle Walding
@tbrnaughttb.bsky.social
· Jul 14
Kyle Walding
@tbrnaughttb.bsky.social
· Jun 10
Kyle Walding
@tbrnaughttb.bsky.social
· Jun 4
Kyle Walding
@tbrnaughttb.bsky.social
· Jun 4
Kyle Walding
@tbrnaughttb.bsky.social
· Jun 3
Kyle Walding
@tbrnaughttb.bsky.social
· Jun 3
Kyle Walding
@tbrnaughttb.bsky.social
· Jun 3
Kyle Walding
@tbrnaughttb.bsky.social
· Jun 3
Kyle Walding
@tbrnaughttb.bsky.social
· Jun 3
Kyle Walding
@tbrnaughttb.bsky.social
· May 31
Kyle Walding
@tbrnaughttb.bsky.social
· May 27

Incipient and Subclinical Tuberculosis: a Clinical Review of Early Stages and Progression of Infection - PubMed
Tuberculosis (TB) is the leading infectious cause of mortality worldwide, due in part to a limited understanding of its clinical pathogenic spectrum of infection and disease. Historically, scientific ...
pubmed.ncbi.nlm.nih.gov
Kyle Walding
@tbrnaughttb.bsky.social
· May 21
Kyle Walding
@tbrnaughttb.bsky.social
· May 19
Kyle Walding
@tbrnaughttb.bsky.social
· May 16
Kyle Walding
@tbrnaughttb.bsky.social
· May 16
Kyle Walding
@tbrnaughttb.bsky.social
· May 16


Kyle Walding
@tbrnaughttb.bsky.social
· May 12
Reposted by Kyle Walding

Kyle Walding
@tbrnaughttb.bsky.social
· Apr 30
Reposted by Kyle Walding
Brad Spellberg
@bradspellberg.bsky.social
· Apr 23
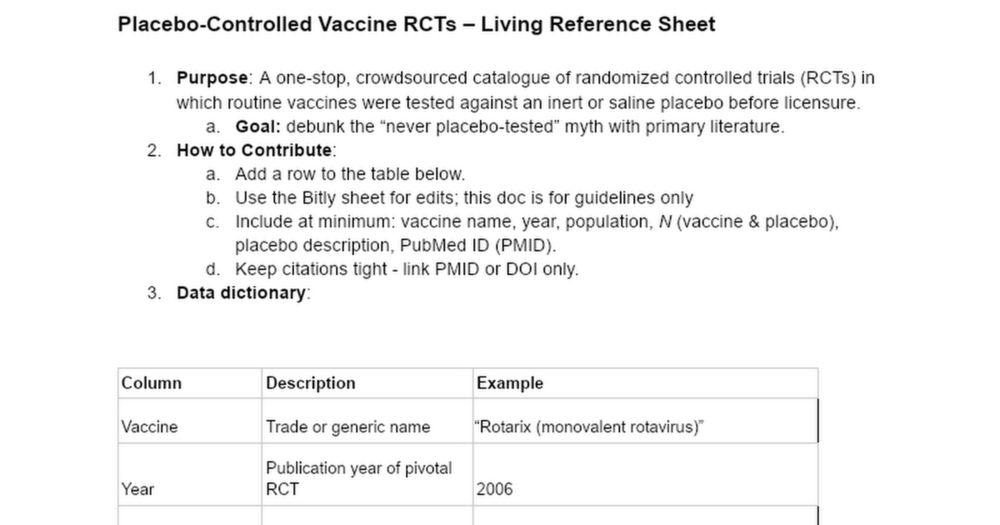
Placebo-Controlled Vaccine RCTs – Living Reference Sheet
Placebo-Controlled Vaccine RCTs – Living Reference Sheet Purpose: A one-stop, crowdsourced catalogue of randomized controlled trials (RCTs) in which routine vaccines were tested against an inert or s...
bit.ly
Kyle Walding
@tbrnaughttb.bsky.social
· Apr 20