



Rachel Bonnifield
@rachelbonnifield.bsky.social
Director of Global Health Policy & Senior Fellow @Cgdev. Global health, lead poisoning, R&D, AMR, pandemic prep, pharma, econ, and development, with a side of foster kittens. Views are my own.
Millions of kids need a life-changing drug that could prevent permanent brain damange from lead poisoning.
The medicine is off-patent, on the WHO Essential Medicine List, and cheap to make.
So why is it still unaffordable & out of reach?
w/Theo Mitchell
www.cgdev.org/blog/million...
The medicine is off-patent, on the WHO Essential Medicine List, and cheap to make.
So why is it still unaffordable & out of reach?
w/Theo Mitchell
www.cgdev.org/blog/million...

Millions of Children Need Life-Changing Lead Poisoning Medicine. Why Isn’t It Affordable?
Children with extreme exposure to lead are at risk of lifelong physical and mental disability. The most practical treatment for this kind of exposure is oral chelation therapy—and we estimate there ar...
www.cgdev.org
November 19, 2025 at 9:42 AM
Millions of kids need a life-changing drug that could prevent permanent brain damange from lead poisoning.
The medicine is off-patent, on the WHO Essential Medicine List, and cheap to make.
So why is it still unaffordable & out of reach?
w/Theo Mitchell
www.cgdev.org/blog/million...
The medicine is off-patent, on the WHO Essential Medicine List, and cheap to make.
So why is it still unaffordable & out of reach?
w/Theo Mitchell
www.cgdev.org/blog/million...
Millions of kids need a life-changing drug that could prevent permanent brain damange from lead poisoning.
The medicine is off-patent, on the WHO Essential Medicine List, and cheap to make.
So why is it still unaffordable & out of reach?
w/Theo Mitchell
www.cgdev.org/blog/million...
The medicine is off-patent, on the WHO Essential Medicine List, and cheap to make.
So why is it still unaffordable & out of reach?
w/Theo Mitchell
www.cgdev.org/blog/million...
Millions of Children Need Life-Changing Lead Poisoning Medicine. Why Isn’t It Affordable?
Children with extreme exposure to lead are at risk of lifelong physical and mental disability. The most practical treatment for this kind of exposure is oral chelation therapy—and we estimate there ar...
www.cgdev.org
November 19, 2025 at 9:42 AM
Millions of kids need a life-changing drug that could prevent permanent brain damange from lead poisoning.
The medicine is off-patent, on the WHO Essential Medicine List, and cheap to make.
So why is it still unaffordable & out of reach?
w/Theo Mitchell
www.cgdev.org/blog/million...
The medicine is off-patent, on the WHO Essential Medicine List, and cheap to make.
So why is it still unaffordable & out of reach?
w/Theo Mitchell
www.cgdev.org/blog/million...
Global lead poisoning makes the cover of the NYT -- documenting how dirty battery recycling in Africa powers the US automobile industry. Important read 👇
www.nytimes.com/interactive/...
www.nytimes.com/interactive/...

The Auto Industry’s Lead Recycling Program is Poisoning People
We documented the toxic fallout of a green technology.
www.nytimes.com
November 18, 2025 at 1:00 PM
Global lead poisoning makes the cover of the NYT -- documenting how dirty battery recycling in Africa powers the US automobile industry. Important read 👇
www.nytimes.com/interactive/...
www.nytimes.com/interactive/...
PEPFAR is at a great American success story at a crossroads.
The Trump Administration's Global Health Strategy offers a broadly reasonable blueprint for PEPFAR's next chapter: more country ownership, deliverty by national governments, and spending cuts. 1/x
The Trump Administration's Global Health Strategy offers a broadly reasonable blueprint for PEPFAR's next chapter: more country ownership, deliverty by national governments, and spending cuts. 1/x
November 14, 2025 at 2:59 PM
PEPFAR is at a great American success story at a crossroads.
The Trump Administration's Global Health Strategy offers a broadly reasonable blueprint for PEPFAR's next chapter: more country ownership, deliverty by national governments, and spending cuts. 1/x
The Trump Administration's Global Health Strategy offers a broadly reasonable blueprint for PEPFAR's next chapter: more country ownership, deliverty by national governments, and spending cuts. 1/x
Reposted by Rachel Bonnifield

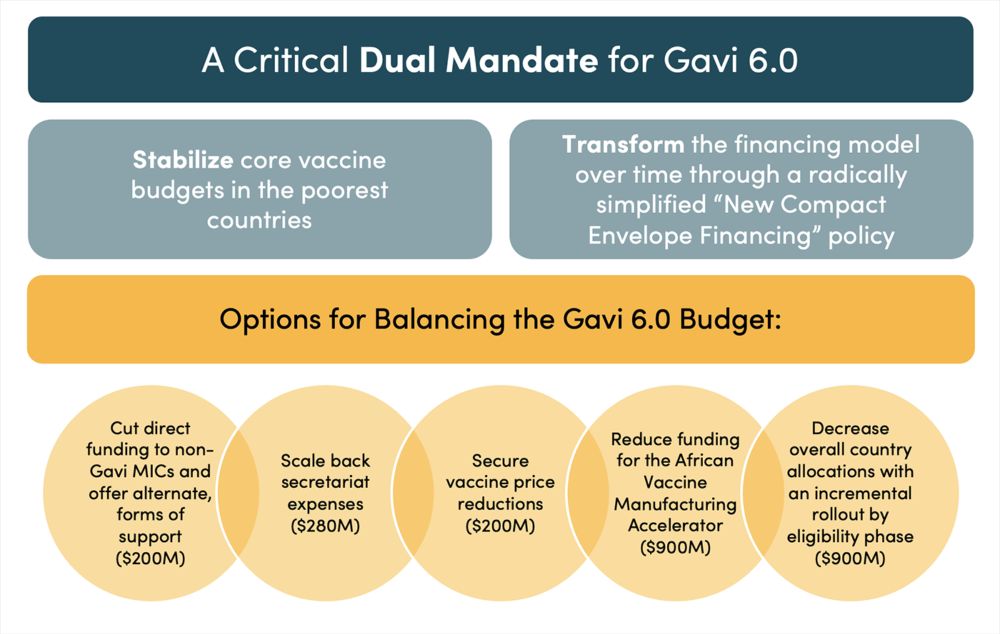
How do you find $2.5 B in savings when every decision has consequences for access to life-saving vaccines? With Center for Global Development colleagues, here are 2 core principles and 5 suggestions. Give it a read and let us know what you think. #gavi
Amid a broader global health financing crisis, @gavi.org faces a $2.5B budget shortfall
Read our new @cgdev.org brief on how Gavi 6.0 can take a bigger leap w @rachelbonnifield.bsky.social @peterbaker17.bsky.social @tomldrake.bsky.social & @orinlevine.bsky.social
www.cgdev.org/publication/...
Read our new @cgdev.org brief on how Gavi 6.0 can take a bigger leap w @rachelbonnifield.bsky.social @peterbaker17.bsky.social @tomldrake.bsky.social & @orinlevine.bsky.social
www.cgdev.org/publication/...
How Gavi 6.0 Can Take a Bigger Leap
Gavi’s board and leadership must stretch scarce resources to fulfill a challenging double mandate: (1) stabilizing immunization outcomes and fiscal solvency in Gavi-eligible countries facing severe he...
www.cgdev.org
July 18, 2025 at 6:48 PM
How do you find $2.5 B in savings when every decision has consequences for access to life-saving vaccines? With Center for Global Development colleagues, here are 2 core principles and 5 suggestions. Give it a read and let us know what you think. #gavi
Reposted by Rachel Bonnifield

Amid a broader global health financing crisis, @gavi.org faces a $2.5B budget shortfall
Read our new @cgdev.org brief on how Gavi 6.0 can take a bigger leap w @rachelbonnifield.bsky.social @peterbaker17.bsky.social @tomldrake.bsky.social & @orinlevine.bsky.social
www.cgdev.org/publication/...
Read our new @cgdev.org brief on how Gavi 6.0 can take a bigger leap w @rachelbonnifield.bsky.social @peterbaker17.bsky.social @tomldrake.bsky.social & @orinlevine.bsky.social
www.cgdev.org/publication/...
How Gavi 6.0 Can Take a Bigger Leap
Gavi’s board and leadership must stretch scarce resources to fulfill a challenging double mandate: (1) stabilizing immunization outcomes and fiscal solvency in Gavi-eligible countries facing severe he...
www.cgdev.org
July 18, 2025 at 2:39 PM
Amid a broader global health financing crisis, @gavi.org faces a $2.5B budget shortfall
Read our new @cgdev.org brief on how Gavi 6.0 can take a bigger leap w @rachelbonnifield.bsky.social @peterbaker17.bsky.social @tomldrake.bsky.social & @orinlevine.bsky.social
www.cgdev.org/publication/...
Read our new @cgdev.org brief on how Gavi 6.0 can take a bigger leap w @rachelbonnifield.bsky.social @peterbaker17.bsky.social @tomldrake.bsky.social & @orinlevine.bsky.social
www.cgdev.org/publication/...
Reposted by Rachel Bonnifield

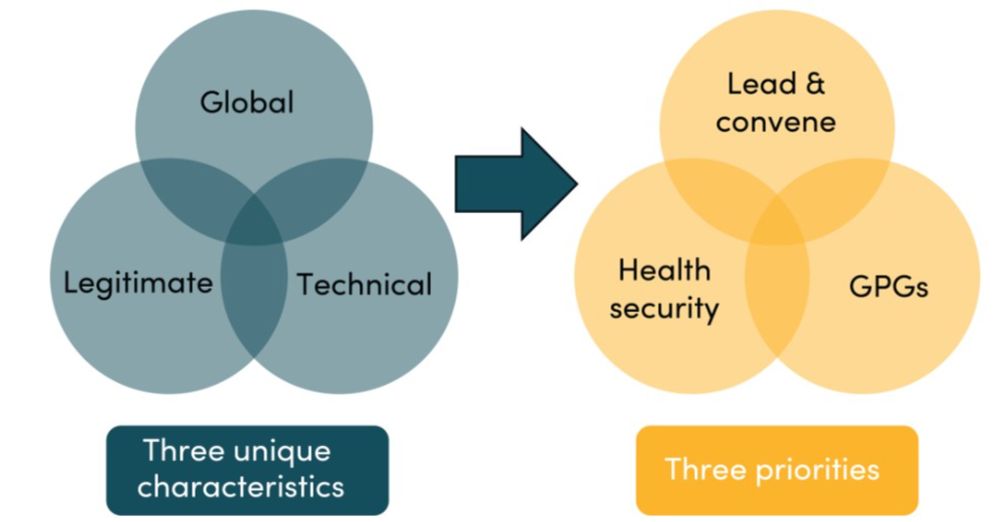
WHO faces immediate fiscal crisis, w/ a 35% budget gap of $1.5bn.
@peterbaker17.bsky.social, @rachelbonnifield.bsky.social, & @jmadankeller.bsky.social argue that WHO’s leadership must chart a path of retrenchment to global leadership, health security, & public goods:
www.cgdev.org/publication/...
@peterbaker17.bsky.social, @rachelbonnifield.bsky.social, & @jmadankeller.bsky.social argue that WHO’s leadership must chart a path of retrenchment to global leadership, health security, & public goods:
www.cgdev.org/publication/...
A Lean World Health Organization for the Global Good
In this brief—the first in the Tough Times, Tough Choices series that will target the major global health and development institutions and their funders—we propose a different approach: radically stre...
www.cgdev.org
July 11, 2025 at 4:29 PM
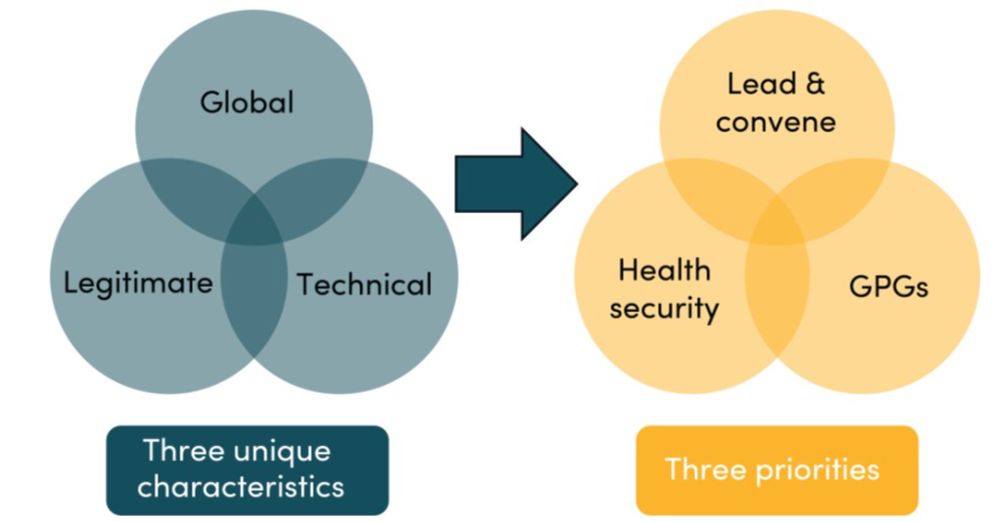
WHO faces immediate fiscal crisis, w/ a 35% budget gap of $1.5bn.
@peterbaker17.bsky.social, @rachelbonnifield.bsky.social, & @jmadankeller.bsky.social argue that WHO’s leadership must chart a path of retrenchment to global leadership, health security, & public goods:
www.cgdev.org/publication/...
@peterbaker17.bsky.social, @rachelbonnifield.bsky.social, & @jmadankeller.bsky.social argue that WHO’s leadership must chart a path of retrenchment to global leadership, health security, & public goods:
www.cgdev.org/publication/...
Reposted by Rachel Bonnifield
1st edition of our @cgdev.org series "Tough Times, Tough Choices" is hot off the press
Facing budget cuts, we argue WHO's leadership must chart a path of retrenchment to a lean @who.int for the global good
w/ @peterbaker17.bsky.social & @rachelbonnifield.bsky.social
www.cgdev.org/publication/...
Facing budget cuts, we argue WHO's leadership must chart a path of retrenchment to a lean @who.int for the global good
w/ @peterbaker17.bsky.social & @rachelbonnifield.bsky.social
www.cgdev.org/publication/...
A Lean World Health Organization for the Global Good
In this brief—the first in the Tough Times, Tough Choices series that will target the major global health and development institutions and their funders—we propose a different approach: radically stre...
www.cgdev.org
July 10, 2025 at 8:01 AM
1st edition of our @cgdev.org series "Tough Times, Tough Choices" is hot off the press
Facing budget cuts, we argue WHO's leadership must chart a path of retrenchment to a lean @who.int for the global good
w/ @peterbaker17.bsky.social & @rachelbonnifield.bsky.social
www.cgdev.org/publication/...
Facing budget cuts, we argue WHO's leadership must chart a path of retrenchment to a lean @who.int for the global good
w/ @peterbaker17.bsky.social & @rachelbonnifield.bsky.social
www.cgdev.org/publication/...
Reposted by Rachel Bonnifield
Cutting US funding for @gavi.org which leads on global vaccination efforts is incredibly shortsighted and misguided
@charlesjkenny.bsky.social & I argued why in this @cgdev.org blog 👇
www.cgdev.org/blog/why-tru...
@charlesjkenny.bsky.social & I argued why in this @cgdev.org blog 👇
www.cgdev.org/blog/why-tru...

June 25, 2025 at 6:48 PM
Cutting US funding for @gavi.org which leads on global vaccination efforts is incredibly shortsighted and misguided
@charlesjkenny.bsky.social & I argued why in this @cgdev.org blog 👇
www.cgdev.org/blog/why-tru...
@charlesjkenny.bsky.social & I argued why in this @cgdev.org blog 👇
www.cgdev.org/blog/why-tru...
Reposted by Rachel Bonnifield

Fantastic news that Switzerland have now submitted the paperwork triggering the start of the process that could eventually lead to better regulation on lead paint exports
ipen.org/news/lead-ch...
ipen.org/news/lead-ch...
June 12, 2025 at 12:48 PM
Fantastic news that Switzerland have now submitted the paperwork triggering the start of the process that could eventually lead to better regulation on lead paint exports
ipen.org/news/lead-ch...
ipen.org/news/lead-ch...
Reposted by Rachel Bonnifield
Starting now! Tune in on CGD YouTube

June 3, 2025 at 5:08 PM
Starting now! Tune in on CGD YouTube
Reposted by Rachel Bonnifield

"In Cleveland, where 20% of children have elevated lead levels, Dave Margolius, director of the Cleveland Department of Public Health say they’ve also lost CDC assistance for lead prevention.
“The percentage of children poisoned by lead in Cleveland is higher than Flint, Michigan was at its peak”"
“The percentage of children poisoned by lead in Cleveland is higher than Flint, Michigan was at its peak”"

White House to Cities: Good Luck Fighting Lead Poisoning
Centers for Disease Control staff cuts leave cities to fight lead poisoning that endangers children without federal help.
wordinblack.com
May 14, 2025 at 1:37 PM
"In Cleveland, where 20% of children have elevated lead levels, Dave Margolius, director of the Cleveland Department of Public Health say they’ve also lost CDC assistance for lead prevention.
“The percentage of children poisoned by lead in Cleveland is higher than Flint, Michigan was at its peak”"
“The percentage of children poisoned by lead in Cleveland is higher than Flint, Michigan was at its peak”"
Reposted by Rachel Bonnifield

The Market for Prescription Drugs Is Broken. Here’s Why Trump’s Executive Order Would Make It Worse
www.cgdev.org/blog/market-...
www.cgdev.org/blog/market-...

The Market for Prescription Drugs Is Broken. Here’s Why Trump’s Executive Order Would Make It Worse
The US pays—by far—the highest prices for on-patent prescription drugs of any country on earth. The White House just issued an executive order purporting to fix this problem. But the proposed solution...
www.cgdev.org
May 13, 2025 at 8:00 PM
The Market for Prescription Drugs Is Broken. Here’s Why Trump’s Executive Order Would Make It Worse
www.cgdev.org/blog/market-...
www.cgdev.org/blog/market-...
Reposted by Rachel Bonnifield
📣New @cgdev.org blog on the latest Trump EO to curb high drug prices
We breakdown why the proposed policy prescription of "reference pricing" is misguided... with a healthy dose of econ101 🤓
w/ @charlesjkenny.bsky.social & @rachelbonnifield.bsky.social
www.cgdev.org/blog/market-...
We breakdown why the proposed policy prescription of "reference pricing" is misguided... with a healthy dose of econ101 🤓
w/ @charlesjkenny.bsky.social & @rachelbonnifield.bsky.social
www.cgdev.org/blog/market-...

The Market for Prescription Drugs Is Broken. Here’s Why Trump’s Executive Order Would Make It Worse
The US pays—by far—the highest prices for on-patent prescription drugs of any country on earth. The White House just issued an executive order purporting to fix this problem. But the proposed solution...
www.cgdev.org
May 13, 2025 at 6:21 PM
📣New @cgdev.org blog on the latest Trump EO to curb high drug prices
We breakdown why the proposed policy prescription of "reference pricing" is misguided... with a healthy dose of econ101 🤓
w/ @charlesjkenny.bsky.social & @rachelbonnifield.bsky.social
www.cgdev.org/blog/market-...
We breakdown why the proposed policy prescription of "reference pricing" is misguided... with a healthy dose of econ101 🤓
w/ @charlesjkenny.bsky.social & @rachelbonnifield.bsky.social
www.cgdev.org/blog/market-...
US drug prices are way too high—but the Trump EO to “fix” them would make things worse for everyone.
We break down the economics of reference pricing here — and explain why it’s a bad approach for the US 👇
With @charlesjkenny.bsky.social and @jmadankeller.bsky.social
www.cgdev.org/blog/market-...
We break down the economics of reference pricing here — and explain why it’s a bad approach for the US 👇
With @charlesjkenny.bsky.social and @jmadankeller.bsky.social
www.cgdev.org/blog/market-...

The Market for Prescription Drugs Is Broken. Here’s Why Trump’s Executive Order Would Make It Worse
The US pays—by far—the highest prices for on-patent prescription drugs of any country on earth. The White House just issued an executive order purporting to fix this problem. But the proposed solution...
www.cgdev.org
May 13, 2025 at 5:53 PM
US drug prices are way too high—but the Trump EO to “fix” them would make things worse for everyone.
We break down the economics of reference pricing here — and explain why it’s a bad approach for the US 👇
With @charlesjkenny.bsky.social and @jmadankeller.bsky.social
www.cgdev.org/blog/market-...
We break down the economics of reference pricing here — and explain why it’s a bad approach for the US 👇
With @charlesjkenny.bsky.social and @jmadankeller.bsky.social
www.cgdev.org/blog/market-...
New Trump EO on drug pricing just dropped and there's...a lot going on there. A breakdown 👇 www.whitehouse.gov/presidential...

Delivering Most-Favored-Nation Prescription Drug Pricing to American Patients
By the authority vested in me as President by the Constitution and the laws of the United States of America, it is hereby ordered: Section 1. Purpose.
www.whitehouse.gov
May 12, 2025 at 4:40 PM
New Trump EO on drug pricing just dropped and there's...a lot going on there. A breakdown 👇 www.whitehouse.gov/presidential...
Feeling *inspired* to renew my Canadian passport 🍁
"I'm going to govern in econometrics" is a winning campaign slogan for the ages.
April 29, 2025 at 6:56 PM
Feeling *inspired* to renew my Canadian passport 🍁
Reposted by Rachel Bonnifield

"I'm going to govern in econometrics" is a winning campaign slogan for the ages.
April 29, 2025 at 2:59 AM
"I'm going to govern in econometrics" is a winning campaign slogan for the ages.
Reposted by Rachel Bonnifield

"We've been left no choice but to this week suspend treatment for 650,000 malnourished women and children — simply because we've run out of commodities and funding," Zlatan Milisic, WFP Country Director in Ethiopia told a Geneva press briefing by video from Addis Ababa.

Malnutrition treatments halted in Ethiopia due to underfunding, WFP says reut.rs/4jB8BVW

April 22, 2025 at 1:05 PM
"We've been left no choice but to this week suspend treatment for 650,000 malnourished women and children — simply because we've run out of commodities and funding," Zlatan Milisic, WFP Country Director in Ethiopia told a Geneva press briefing by video from Addis Ababa.
Reposted by Rachel Bonnifield

Reposted by Rachel Bonnifield

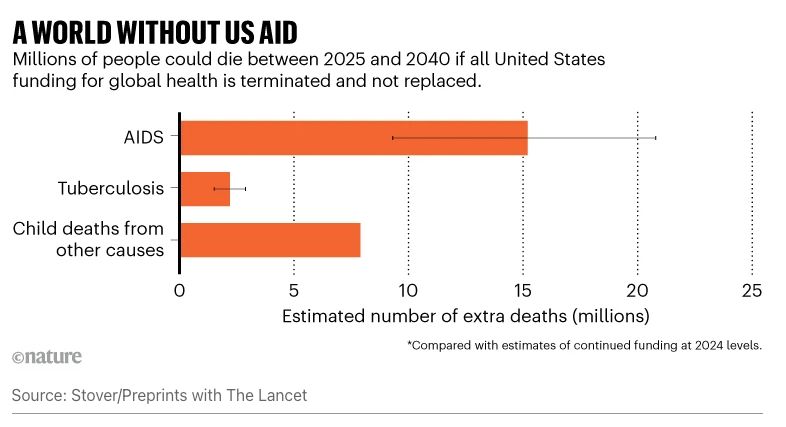
New preprint finding that eliminating US global health funding over the next fifteen years would cause:
- 15.2m deaths from AIDS
- 2.2m deaths from TB
- 7.9 additional child deaths
- 15.2m deaths from AIDS
- 2.2m deaths from TB
- 7.9 additional child deaths
April 17, 2025 at 8:32 PM
New preprint finding that eliminating US global health funding over the next fifteen years would cause:
- 15.2m deaths from AIDS
- 2.2m deaths from TB
- 7.9 additional child deaths
- 15.2m deaths from AIDS
- 2.2m deaths from TB
- 7.9 additional child deaths
Reposted by Rachel Bonnifield

CNN story on lead poisoning & HHS/CDC's inability to act: Wisconsin asked the CDC for help with lead poisoning cases in Milwaukee but CDC had to cancel because HHS Secretary laid off all the CDC lead poisoning experts! Screenshot below of Ex CDC Director Tom Frieden's '09-'17 comments today #medsky

April 10, 2025 at 7:54 PM
CNN story on lead poisoning & HHS/CDC's inability to act: Wisconsin asked the CDC for help with lead poisoning cases in Milwaukee but CDC had to cancel because HHS Secretary laid off all the CDC lead poisoning experts! Screenshot below of Ex CDC Director Tom Frieden's '09-'17 comments today #medsky
Reposted by Rachel Bonnifield
Non-toxic options to lead chromate—a toxic paint pigment—have existed for years.
But @rorytodd98.bsky.social, @leecrawfurd.bsky.social, & @rachelbonnifield.bsky.social find that rich countries like the US & UK still export it to poorer nations, despite banning/restricting it at home:
bit.ly/4jusvlJ
But @rorytodd98.bsky.social, @leecrawfurd.bsky.social, & @rachelbonnifield.bsky.social find that rich countries like the US & UK still export it to poorer nations, despite banning/restricting it at home:
bit.ly/4jusvlJ

Rich Countries Are Exporting Thousands of Tons of Toxic Paint Pigment to Poor Countries
One in three children globally suffer from lead poisoning, which harms their health and educational development. While there’s a lot we still don’t know about where exposure comes from, most experts w...
bit.ly
April 10, 2025 at 2:43 PM
Non-toxic options to lead chromate—a toxic paint pigment—have existed for years.
But @rorytodd98.bsky.social, @leecrawfurd.bsky.social, & @rachelbonnifield.bsky.social find that rich countries like the US & UK still export it to poorer nations, despite banning/restricting it at home:
bit.ly/4jusvlJ
But @rorytodd98.bsky.social, @leecrawfurd.bsky.social, & @rachelbonnifield.bsky.social find that rich countries like the US & UK still export it to poorer nations, despite banning/restricting it at home:
bit.ly/4jusvlJ
I step away from my feed and try to do real work for 15 freaking minutes...
April 9, 2025 at 5:40 PM
I step away from my feed and try to do real work for 15 freaking minutes...
Reposted by Rachel Bonnifield
In DC for spring meetings? Join me & @clemencelanders.bsky.social on Wed Apr 23 for a @cgdev.org event on how multilateral funds can evolve in the face of shrinking resources and growing needs
RSVP ➡️ www.cgdev.org/event/how-do...
RSVP ➡️ www.cgdev.org/event/how-do...
April 9, 2025 at 5:09 PM
In DC for spring meetings? Join me & @clemencelanders.bsky.social on Wed Apr 23 for a @cgdev.org event on how multilateral funds can evolve in the face of shrinking resources and growing needs
RSVP ➡️ www.cgdev.org/event/how-do...
RSVP ➡️ www.cgdev.org/event/how-do...