



Iain Bressendorff, MD PhD
@ibressendorff.bsky.social
Nephrologist, clinical trials, PRIMETIME study.
CKD-MBD, GN, DKD, amateur 80’s musician, MTG
#NephSky
CKD-MBD, GN, DKD, amateur 80’s musician, MTG
#NephSky
Reposted by Iain Bressendorff, MD PhD

Join the Filtrate and Jon Barratt as he takes an IgAN inspired victory lap
FF 86 Atacicept for IgAN
www.nephjc.com/freelyfilter...
FF 86 Atacicept for IgAN
www.nephjc.com/freelyfilter...

FF 86 Atacicept for IgAN with Jon Barratt — NephJC
FF 86 Atacicept for IgAN with Jon Barratt
www.nephjc.com
November 28, 2025 at 3:01 PM
Join the Filtrate and Jon Barratt as he takes an IgAN inspired victory lap
FF 86 Atacicept for IgAN
www.nephjc.com/freelyfilter...
FF 86 Atacicept for IgAN
www.nephjc.com/freelyfilter...
I’m a little shocked at this review of resistant hypertension in CKD.
academic.oup.com/ckj/advance-...
- Weird take on BP targets (there are other trials besides SPRINT)
- Thiazides don’t work in CKD, except chlorthalidone (demonstrably false)
- Don’t use spiro if eGFR <45 because hyperK ?!?!?
1/2
academic.oup.com/ckj/advance-...
- Weird take on BP targets (there are other trials besides SPRINT)
- Thiazides don’t work in CKD, except chlorthalidone (demonstrably false)
- Don’t use spiro if eGFR <45 because hyperK ?!?!?
1/2

2025 Update on resistant hypertension in CKD: where do we stand and where do we go?
Abstract. Resistant hypertension is highly prevalent among individuals with chronic kidney disease (CKD) and is closely associated with accelerated decline
academic.oup.com
November 23, 2025 at 3:40 PM
I’m a little shocked at this review of resistant hypertension in CKD.
academic.oup.com/ckj/advance-...
- Weird take on BP targets (there are other trials besides SPRINT)
- Thiazides don’t work in CKD, except chlorthalidone (demonstrably false)
- Don’t use spiro if eGFR <45 because hyperK ?!?!?
1/2
academic.oup.com/ckj/advance-...
- Weird take on BP targets (there are other trials besides SPRINT)
- Thiazides don’t work in CKD, except chlorthalidone (demonstrably false)
- Don’t use spiro if eGFR <45 because hyperK ?!?!?
1/2
Reposted by Iain Bressendorff, MD PhD

7. Personal level. Beyond his talent and expertise, I met an extraordinary man. Humble, altruistic, wise, friendly, and with a great sense of humor. I brought him a vacuolar cast tie as a present and he wore it proudly right away 🤩

November 21, 2025 at 5:24 PM
7. Personal level. Beyond his talent and expertise, I met an extraordinary man. Humble, altruistic, wise, friendly, and with a great sense of humor. I brought him a vacuolar cast tie as a present and he wore it proudly right away 🤩
Reposted by Iain Bressendorff, MD PhD
1/n Recently attended an international congress about Urinalysis in Santiago, Chile 🇨🇱. I was expecting a small meeting. I was wrong. Pleasantly surprised with the size of the meeting and the energy and interest from the participants. Let me share the highlights of my experience:

November 21, 2025 at 5:24 PM
1/n Recently attended an international congress about Urinalysis in Santiago, Chile 🇨🇱. I was expecting a small meeting. I was wrong. Pleasantly surprised with the size of the meeting and the energy and interest from the participants. Let me share the highlights of my experience:
Reposted by Iain Bressendorff, MD PhD
Diagnosis unmasked. Young F with 2g proteinuria, weak +dsDNA. Membranous pattern, IF with C3 dominant staining. Pronase IF --> IgG-k. Membranous-like glomerulopathy with masked monotypic IgG-k deposits. Considered to be autoimmune; not MGRS. #renalpath #pathsky #nephsky.




November 20, 2025 at 1:01 PM
Diagnosis unmasked. Young F with 2g proteinuria, weak +dsDNA. Membranous pattern, IF with C3 dominant staining. Pronase IF --> IgG-k. Membranous-like glomerulopathy with masked monotypic IgG-k deposits. Considered to be autoimmune; not MGRS. #renalpath #pathsky #nephsky.
Reposted by Iain Bressendorff, MD PhD
Neuronal proteins show up in so many of our proteomics and mass spectrometry experiments on renal tissues and cells, especially the podocyte! Larry Beck and Laith Al-Rabadi discuss this in the context of MN here.

Neuronal Proteins as Antigenic Targets in Membranous Nephropathy
Abstract. Context: The discovery of new target antigens in membranous nephropathy (MN) has revealed new disease phenotypes and, in some cases, has suggested mechanisms of disease shared by two concurr...
karger.com
November 20, 2025 at 5:44 AM
Neuronal proteins show up in so many of our proteomics and mass spectrometry experiments on renal tissues and cells, especially the podocyte! Larry Beck and Laith Al-Rabadi discuss this in the context of MN here.
Reposted by Iain Bressendorff, MD PhD

Nothing works in dialysis - except fis oil. Truly amazing data from the PISCES. Should we begin perscribimg fish oil supplements to all our dialysis patients? In spite of my somewhat sceptical priors, I think the answer should be “yes” #NephSky #KidneyWk #nephrology
November 9, 2025 at 11:26 AM
Nothing works in dialysis - except fis oil. Truly amazing data from the PISCES. Should we begin perscribimg fish oil supplements to all our dialysis patients? In spite of my somewhat sceptical priors, I think the answer should be “yes” #NephSky #KidneyWk #nephrology
Reposted by Iain Bressendorff, MD PhD

Reposted by Iain Bressendorff, MD PhD

What mechanisms drive checkpoint inhibitor-associated interstitial nephritis (ICI-AIN)?
In our preprint, we identify CD8 T cells as a central player, inducing a proinflammatory myeloid cell state by IFNg and structuring lymphoid aggregates by CXCL13.
www.biorxiv.org/content/10.1...
1/n
#Nephsky 🧪
In our preprint, we identify CD8 T cells as a central player, inducing a proinflammatory myeloid cell state by IFNg and structuring lymphoid aggregates by CXCL13.
www.biorxiv.org/content/10.1...
1/n
#Nephsky 🧪

November 5, 2025 at 6:24 PM
What mechanisms drive checkpoint inhibitor-associated interstitial nephritis (ICI-AIN)?
In our preprint, we identify CD8 T cells as a central player, inducing a proinflammatory myeloid cell state by IFNg and structuring lymphoid aggregates by CXCL13.
www.biorxiv.org/content/10.1...
1/n
#Nephsky 🧪
In our preprint, we identify CD8 T cells as a central player, inducing a proinflammatory myeloid cell state by IFNg and structuring lymphoid aggregates by CXCL13.
www.biorxiv.org/content/10.1...
1/n
#Nephsky 🧪
Reposted by Iain Bressendorff, MD PhD
After a 40 minute handa on session where my station worked on kidney US we are back in the lecture room for a talk on lung ultrasound by Nathaniel Reisinger #KidneyWk
November 5, 2025 at 4:10 PM
After a 40 minute handa on session where my station worked on kidney US we are back in the lecture room for a talk on lung ultrasound by Nathaniel Reisinger #KidneyWk
Reposted by Iain Bressendorff, MD PhD

I enjoyed the Observer this morning @drjennings.bsky.social
In my considered view politicians and public bodies should not be on Twitter is for the same reason that a candidate should not attend a townhall meeting where he was put on a lower chair and very loud music played whenever he spoke.
In my considered view politicians and public bodies should not be on Twitter is for the same reason that a candidate should not attend a townhall meeting where he was put on a lower chair and very loud music played whenever he spoke.
November 2, 2025 at 7:16 AM
I enjoyed the Observer this morning @drjennings.bsky.social
In my considered view politicians and public bodies should not be on Twitter is for the same reason that a candidate should not attend a townhall meeting where he was put on a lower chair and very loud music played whenever he spoke.
In my considered view politicians and public bodies should not be on Twitter is for the same reason that a candidate should not attend a townhall meeting where he was put on a lower chair and very loud music played whenever he spoke.
Reposted by Iain Bressendorff, MD PhD
Clinic visit, pt w/type 2 diabetes + nephrotic range proteinuria. Persistent hematuria noted (normal cysto 3 mo ago) not c/w diabetic nephropathy. #UrinarySediment 🔬is performed: numerous acanthocytes and a few WBC casts. Serum IgA elevated. Normal C3/C4. Other tests pending. Kidney biopsy planned




October 23, 2025 at 3:46 AM
Clinic visit, pt w/type 2 diabetes + nephrotic range proteinuria. Persistent hematuria noted (normal cysto 3 mo ago) not c/w diabetic nephropathy. #UrinarySediment 🔬is performed: numerous acanthocytes and a few WBC casts. Serum IgA elevated. Normal C3/C4. Other tests pending. Kidney biopsy planned
Reposted by Iain Bressendorff, MD PhD
New episode of Freely Filtered with @brendonneuen.bsky.social @hswapnil.medsky.social @captainchloride.bsky.social @sophia-kidney.bsky.social and author Muth Vaduganathan discussing the CONVINCE trial
www.nephjc.com/freelyfilter...
With chapters, refs, and pictures
www.nephjc.com/freelyfilter...
With chapters, refs, and pictures



October 21, 2025 at 12:11 PM
New episode of Freely Filtered with @brendonneuen.bsky.social @hswapnil.medsky.social @captainchloride.bsky.social @sophia-kidney.bsky.social and author Muth Vaduganathan discussing the CONVINCE trial
www.nephjc.com/freelyfilter...
With chapters, refs, and pictures
www.nephjc.com/freelyfilter...
With chapters, refs, and pictures
A little opinion piece on the relationship between serum calcification propensity (T50) and progressive CAC in kidney transplant recipients 🤓
www.kireports.org/article/S246...
www.kireports.org/article/S246...

T50 and Calcification Progression in Kidney Transplant Recipients: Does it have to be “bad” to be useful?
The increased risk of cardiovascular disease (CVD) among kidney transplant recipients
(KTR)1 is challenging for the treating physician. For KTR, CVD risk remains higher
than for individuals with simil...
www.kireports.org
September 27, 2025 at 9:27 AM
A little opinion piece on the relationship between serum calcification propensity (T50) and progressive CAC in kidney transplant recipients 🤓
www.kireports.org/article/S246...
www.kireports.org/article/S246...
Reposted by Iain Bressendorff, MD PhD

And it’s live
Iptacopan in C3GN makes it to @thelancet.com
www.thelancet.com/journals/lan...
#NephSky
Iptacopan in C3GN makes it to @thelancet.com
www.thelancet.com/journals/lan...
#NephSky
September 26, 2025 at 9:37 AM
And it’s live
Iptacopan in C3GN makes it to @thelancet.com
www.thelancet.com/journals/lan...
#NephSky
Iptacopan in C3GN makes it to @thelancet.com
www.thelancet.com/journals/lan...
#NephSky
Reposted by Iain Bressendorff, MD PhD
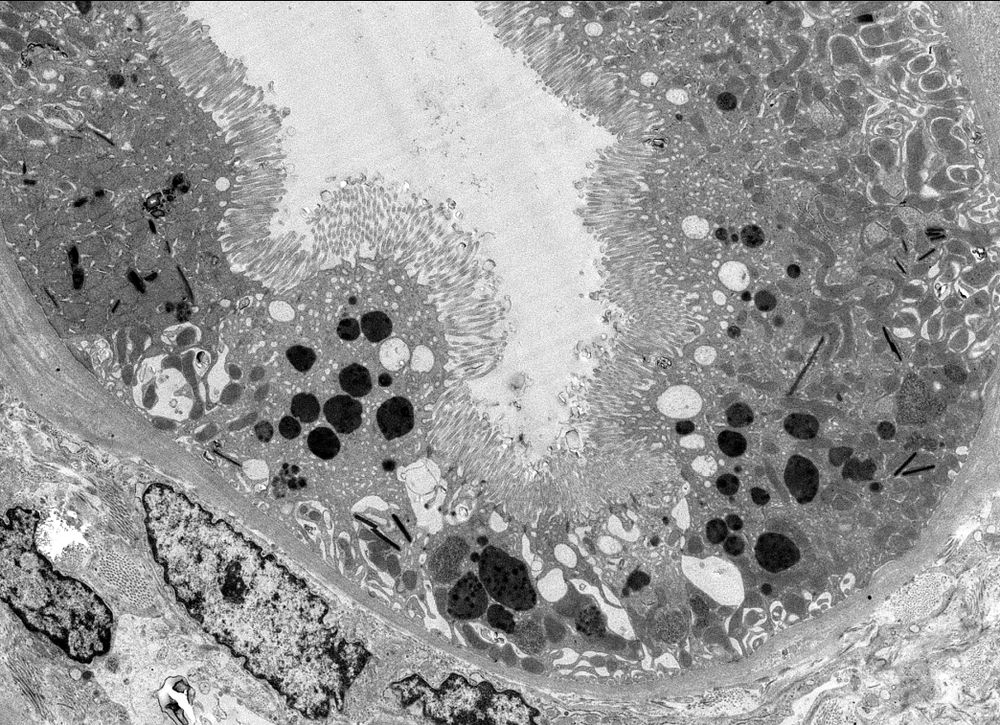
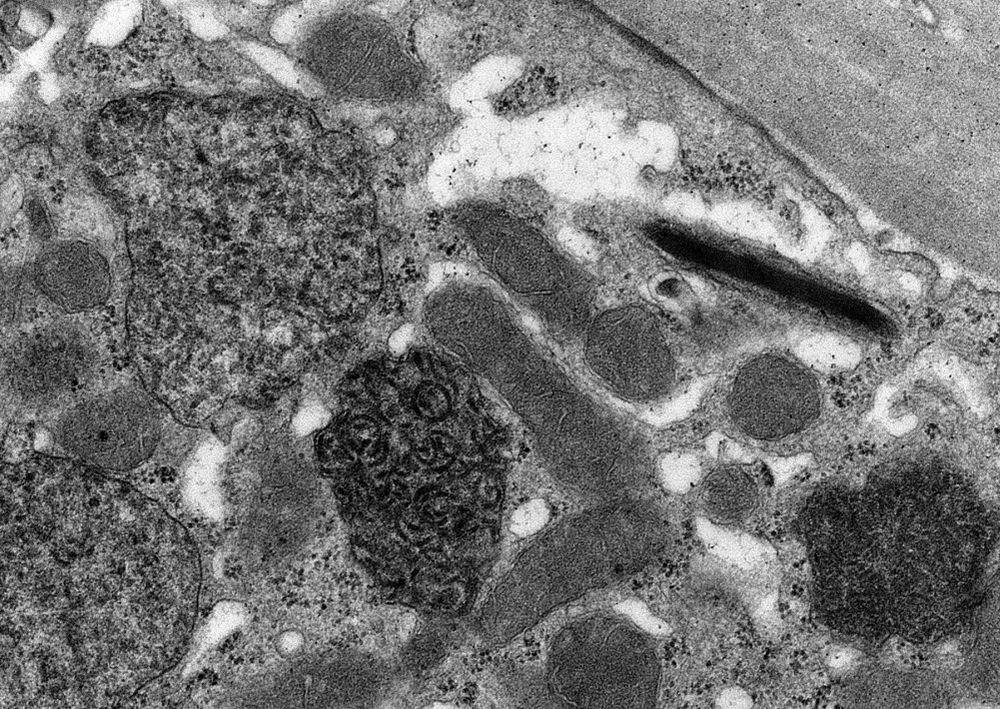
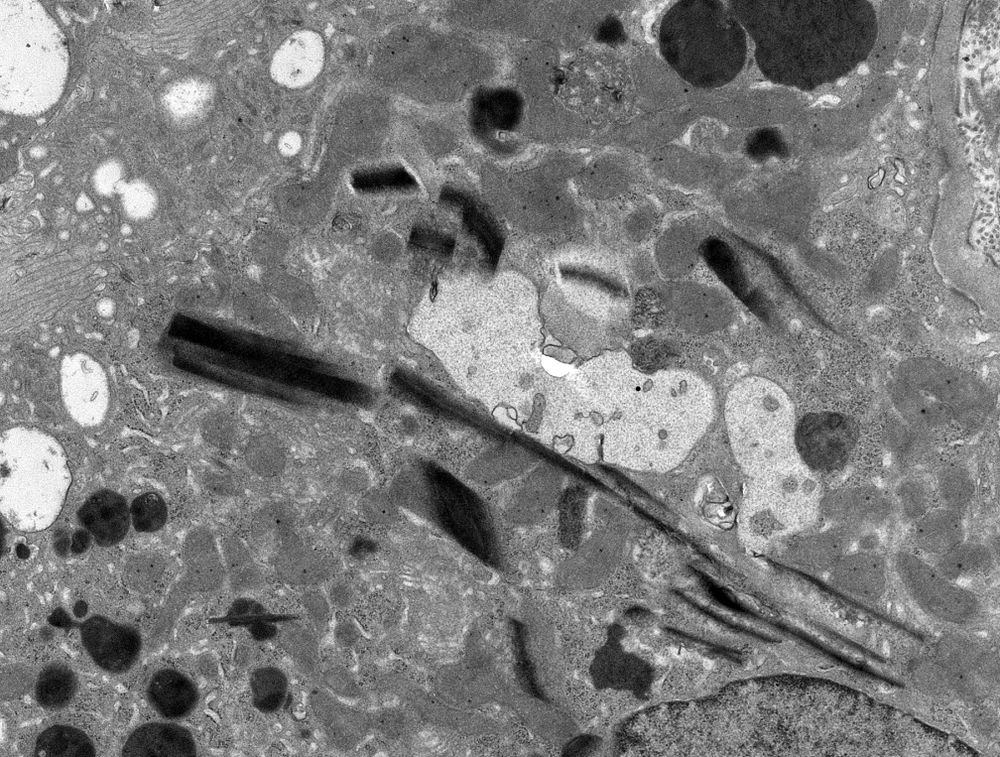
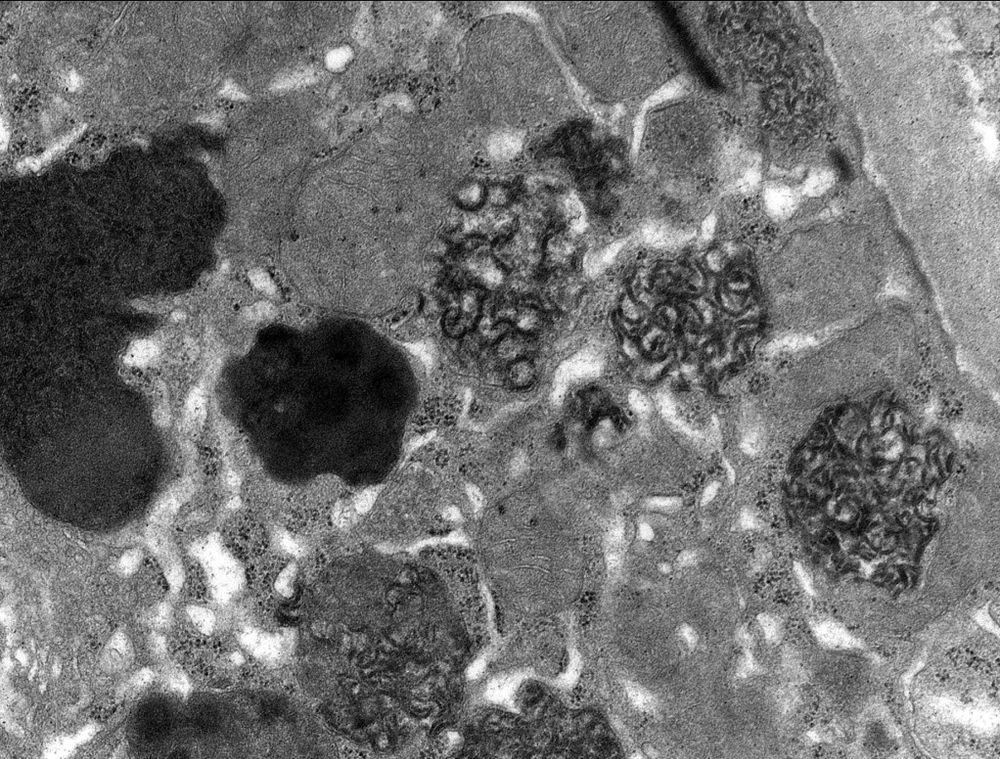
Wide variety of morphologies in this case of crystalline light chain proximal tubulopathy: mottle lysosomes, crystals, and fibrils. #renalpath #nephsky #pathsky
August 6, 2025 at 9:32 PM
Wide variety of morphologies in this case of crystalline light chain proximal tubulopathy: mottle lysosomes, crystals, and fibrils. #renalpath #nephsky #pathsky
Reposted by Iain Bressendorff, MD PhD

Have hyperglycemia (and other DM badness) been hiding in plain sight in ESKD?
Probably.
Great study using CGMs in ESKD.
Pts with treated DM, mean TIR only 43% while mean HbA1c was 7.0%
journals.lww.com/jasn/abstrac...
Probably.
Great study using CGMs in ESKD.
Pts with treated DM, mean TIR only 43% while mean HbA1c was 7.0%
journals.lww.com/jasn/abstrac...

Glycemia Assessed by Continuous Glucose Monitoring among... : Journal of the American Society of Nephrology
ilure and its treatments disrupt glucose homeostasis in ways that may promote both hyperglycemia and hypoglycemia. Continuous glucose monitoring (CGM) delineates detailed glycemic profiles, but publis...
journals.lww.com
September 13, 2025 at 7:16 PM
Have hyperglycemia (and other DM badness) been hiding in plain sight in ESKD?
Probably.
Great study using CGMs in ESKD.
Pts with treated DM, mean TIR only 43% while mean HbA1c was 7.0%
journals.lww.com/jasn/abstrac...
Probably.
Great study using CGMs in ESKD.
Pts with treated DM, mean TIR only 43% while mean HbA1c was 7.0%
journals.lww.com/jasn/abstrac...
Reposted by Iain Bressendorff, MD PhD
RIP Nicolas Madias
Of the Adrogue-Madias formula and much more
I don’t know he wrote three textbooks as a medical student!
www.kidney-international.org/article/S008...
In @kidneyint.bsky.social
#NephSky
Of the Adrogue-Madias formula and much more
I don’t know he wrote three textbooks as a medical student!
www.kidney-international.org/article/S008...
In @kidneyint.bsky.social
#NephSky

August 23, 2025 at 1:22 AM
RIP Nicolas Madias
Of the Adrogue-Madias formula and much more
I don’t know he wrote three textbooks as a medical student!
www.kidney-international.org/article/S008...
In @kidneyint.bsky.social
#NephSky
Of the Adrogue-Madias formula and much more
I don’t know he wrote three textbooks as a medical student!
www.kidney-international.org/article/S008...
In @kidneyint.bsky.social
#NephSky
Reposted by Iain Bressendorff, MD PhD

Now online in @ndt-era.bsky.social
Perlecan is a novel target of autoantibodies in anti-glomerular basement membrane disease
🧐Triple-positive pts (anti-type IV collagen, -laminin 521, and -perlecan) = highest prevalence of lung hemorrhage and ESKD
▶️ academic.oup.com/ndt/article-...
Perlecan is a novel target of autoantibodies in anti-glomerular basement membrane disease
🧐Triple-positive pts (anti-type IV collagen, -laminin 521, and -perlecan) = highest prevalence of lung hemorrhage and ESKD
▶️ academic.oup.com/ndt/article-...

August 12, 2025 at 5:27 AM
Now online in @ndt-era.bsky.social
Perlecan is a novel target of autoantibodies in anti-glomerular basement membrane disease
🧐Triple-positive pts (anti-type IV collagen, -laminin 521, and -perlecan) = highest prevalence of lung hemorrhage and ESKD
▶️ academic.oup.com/ndt/article-...
Perlecan is a novel target of autoantibodies in anti-glomerular basement membrane disease
🧐Triple-positive pts (anti-type IV collagen, -laminin 521, and -perlecan) = highest prevalence of lung hemorrhage and ESKD
▶️ academic.oup.com/ndt/article-...
Does anyone have experience with RTX for anti-GBM disease?
Specifically, elderly/frail patients with anuria and no DAH. Kidneys lost, but high risk with CYC. Systematic review in KI Reports doesn’t entirely answer my Q
@juancarlosqvelez.bsky.social
@kronbichlerlab.bsky.social
@lastwalsh.bsky.social
Specifically, elderly/frail patients with anuria and no DAH. Kidneys lost, but high risk with CYC. Systematic review in KI Reports doesn’t entirely answer my Q
@juancarlosqvelez.bsky.social
@kronbichlerlab.bsky.social
@lastwalsh.bsky.social
August 13, 2025 at 10:40 AM
Does anyone have experience with RTX for anti-GBM disease?
Specifically, elderly/frail patients with anuria and no DAH. Kidneys lost, but high risk with CYC. Systematic review in KI Reports doesn’t entirely answer my Q
@juancarlosqvelez.bsky.social
@kronbichlerlab.bsky.social
@lastwalsh.bsky.social
Specifically, elderly/frail patients with anuria and no DAH. Kidneys lost, but high risk with CYC. Systematic review in KI Reports doesn’t entirely answer my Q
@juancarlosqvelez.bsky.social
@kronbichlerlab.bsky.social
@lastwalsh.bsky.social
Reposted by Iain Bressendorff, MD PhD

Amazing! New species = new DNA to sequence = new knowledge = new breakthroughs at the horizon . Science won’t stop

This surprisingly relaxing footage is from SIX MILES under the ocean – and it’s the deepest ecosystem yet discovered
August 1, 2025 at 7:11 PM
Amazing! New species = new DNA to sequence = new knowledge = new breakthroughs at the horizon . Science won’t stop
Reposted by Iain Bressendorff, MD PhD
Isidore Edelman, father of the Edelman formula was a victim of McCarthyism. Lost his grant and federal funding after being accused of being Red. The American Heart Association stepped up to back fill his funding which allowed him to continue his work on salt and water



July 26, 2025 at 5:15 PM
Isidore Edelman, father of the Edelman formula was a victim of McCarthyism. Lost his grant and federal funding after being accused of being Red. The American Heart Association stepped up to back fill his funding which allowed him to continue his work on salt and water
Reposted by Iain Bressendorff, MD PhD

We often now hear the term “Bayesian borrowing” in trials. But what is Bayesian borrowing and what are the pros and cons around its use? 1/6
#MethodologyMonday #122
#MethodologyMonday #122
July 21, 2025 at 7:10 AM
We often now hear the term “Bayesian borrowing” in trials. But what is Bayesian borrowing and what are the pros and cons around its use? 1/6
#MethodologyMonday #122
#MethodologyMonday #122
Reposted by Iain Bressendorff, MD PhD

Reduction in all-cause hospitalisation driven by fewer admissions for:
- Cardiac
- Renal
- Metabolic disorders, and
- Infections
Interestingly reduction in infections also observed with semaglutide in the FLOW trial - could GDMT improve physical resilience & susceptibility to infections?
- Cardiac
- Renal
- Metabolic disorders, and
- Infections
Interestingly reduction in infections also observed with semaglutide in the FLOW trial - could GDMT improve physical resilience & susceptibility to infections?

July 15, 2025 at 9:16 PM
Reduction in all-cause hospitalisation driven by fewer admissions for:
- Cardiac
- Renal
- Metabolic disorders, and
- Infections
Interestingly reduction in infections also observed with semaglutide in the FLOW trial - could GDMT improve physical resilience & susceptibility to infections?
- Cardiac
- Renal
- Metabolic disorders, and
- Infections
Interestingly reduction in infections also observed with semaglutide in the FLOW trial - could GDMT improve physical resilience & susceptibility to infections?
In resistant HTN guidelines say RAASi + CCB + thiazide followed by spiro. When BP at target, do you try discontinuing the first 3 and ramp up spiro? Or leave them on 4 drugs?
(obviously first rule out primary hyperaldo)
@hswapnil.medsky.social @drjmluther.bsky.social @jordybc.bsky.social
(obviously first rule out primary hyperaldo)
@hswapnil.medsky.social @drjmluther.bsky.social @jordybc.bsky.social
July 15, 2025 at 3:40 PM
In resistant HTN guidelines say RAASi + CCB + thiazide followed by spiro. When BP at target, do you try discontinuing the first 3 and ramp up spiro? Or leave them on 4 drugs?
(obviously first rule out primary hyperaldo)
@hswapnil.medsky.social @drjmluther.bsky.social @jordybc.bsky.social
(obviously first rule out primary hyperaldo)
@hswapnil.medsky.social @drjmluther.bsky.social @jordybc.bsky.social